
Why Smart People Fall for the Biggest Lies
We laugh at the fact that doctors once promoted cigarettes and lobotomies. But one day, future generations will laugh at us too. What are we blindly trusting today?


The following information is based on a report originally published by A Midwestern Doctor. Key details have been streamlined and editorialized for clarity and impact. Read the original report here.
In the 1930s to the early 60s, Americans were convinced smoking was healthy.
Doctors proudly appeared in cigarette ads. “More doctors smoke Camels than any other cigarette.”
The public was given a clear message: If physicians smoked themselves, how dangerous could it possibly be?
At its peak, more than 42% of American adults smoked, with rates among men climbing as high as 50–57%.
Business was booming. But behind the scenes, tobacco companies already knew smoking was linked to deadly disease.
Internal research pointed to the dangers early, yet the industry spent years funding doubt, attacking critics, and delaying public awareness long enough to keep the machine running.
Then came January 11, 1964.
The U.S. Surgeon General released the report that changed everything: smoking causes lung cancer and other deadly illnesses.
Almost overnight, one of the most trusted health narratives in America began to collapse.
And it wasn’t the only one.
In the 1940s and 1950s, lobotomies were celebrated as a revolutionary treatment for mental illness. Walter Freeman traveled the country performing thousands of “ice-pick” procedures, sometimes in minutes, sometimes on children.
The technique even earned a Nobel Prize.
Years later, it was widely condemned as barbaric, after leaving countless patients permanently damaged.
Today, we look back at both eras with disbelief and wonder how entire generations came to trust that later proved so catastrophically wrong.
But the more uncomfortable question is harder to escape:
How many medical “certainties” we trust today will future generations one day look back on the same way?
We hold thousands of assumptions we never question.
Most of them are fine. The dangerous ones are the unquestioned assumptions that aren’t.
This is about what it actually looks like to prioritize truth over being right.
Including when that means publicly correcting something you’ve believed for decades.
Let’s start with a story.
For decades, a widely repeated narrative has appeared in critiques of Western medicine:
That 19th century surgeon James Marion Sims performed experimental gynecological surgeries on enslaved black women without anesthesia—using them as test subjects before performing the same procedures on white women, with anesthesia.
It felt obviously, viscerally wrong. Most people never questioned it.
They just react to it.

As it turns out, what the historical record actually shows is considerably different.
The condition Sims treated—vesicovaginal fistula—was devastating and had no cure at the time. Suffering women were desperate for relief and willingly consented to the procedures.
Ether was brand new, highly controversial, and carried real risks. Sims and other surgeons of the era didn’t believe the pain of these specific operations justified those risks—and applied the same standard regardless of the patient’s race.
The women he worked with helped each other through their recoveries, assisted in surgeries, and pushed him to continue when he wanted to stop. He acknowledged his debt to them publicly. He operated at his own expense.
The narrative most people know about James Marion Sims had been assembled to support a political argument, not drawn from the historical record. And in 2018, after significant protest, his statue in New York City was removed.

This information comes from the work of medical researcher A Midwestern Doctor. For all the sources and details, read the full report below.
Sensitivity, Specificity, and the Art of Seeking Truth

The honest question that follows is as necessary as it is uncomfortable:
Why had this narrative never been questioned?
It was emotionally triggering enough to absorb whole.
It confirmed something already believed.
And it had been repeated—for decades—without obvious attempts to verify it.

You may recall that in the mid-1990s, chain emails swept the internet.
Compelling, shocking stories—sent by someone you trusted—designed to be forwarded before you stopped to think about it.
Virtually every single one of them was demonstrably fake.
But people kept forwarding them anyway. Because the emotional compulsion to share arrives before the analytical impulse to verify.
That’s exactly how they were designed.
The rule that emerged then still hasn’t failed: if the improbable events in a viral story are too perfectly lined up, it’s probably fake.

The Sims narrative followed this pattern.
It was emotionally triggering enough to be absorbed whole. It confirmed something already believed. Specificity collapsed.
So it was never questioned. It simply… was.

Every social group applies a lower standard of proof to narratives that confirm what they already believe.
Most people are excellent at noticing this in the other group.
But almost no one applies the same scrutiny to their own.
And that’s where we go wrong.
Medicine happens to be a particularly significant case of this phenomenon. The medical field readily absorbs false narratives that support its prevailing biases—while reflexively dismissing competing paradigms regardless of their evidence base.
This isn’t unique to medicine. It is, however, obviously more consequential there than in almost any other domain.

In medicine, there’s a concept called sensitivity and specificity.
Sensitivity is how reliably a test identifies what it’s looking for. Specificity is how reliably it avoids false positives.
Every diagnostic test involves a tradeoff between them. Improve one, and you typically worsen the other.
The COVID PCR tests were designed with maximum sensitivity—to miss no cases of infection. The result: so many false positives that large portions of the population concluded the tests were a joke.
Sensitivity without sufficient specificity produces noise.

This framework extends far beyond diagnostic tests.
Criminal justice is a great example. Prioritize sensitivity—catching as many criminals as possible—and you get authoritarian policing and wrongful imprisonment. Prioritize specificity—protecting the innocent from false accusation—and violent crime rises as fewer offenders face consequences.
Political polarization tends to lock each side onto one end of this spectrum, each excellent at identifying the costs of the other’s position and incapable of seeing the costs of their own.

The more interesting application is what this framework reveals about how we filter reality every day—and why most of us are running cognitive filters we never actually chose.
A Midwestern Doctor’s full article is an important read.
Sensitivity, Specificity, and the Art of Seeking Truth
Every day, every person is unconsciously screening out enormous amounts of information while focusing on what their mind has decided matters.
This filtering is almost never chosen deliberately. It operates below our awareness. And it can absolutely be externally hijacked—marketing and propaganda function precisely by directing what you focus on and what you ignore.
The people who consciously choose how their minds filter reality—who deliberately calibrate what they let in and what they dismiss—tend to be significantly more successful and happy in life.

A Midwestern Doctor’s DMSO series illustrates what genuinely deliberate filtering looks like at its extreme.
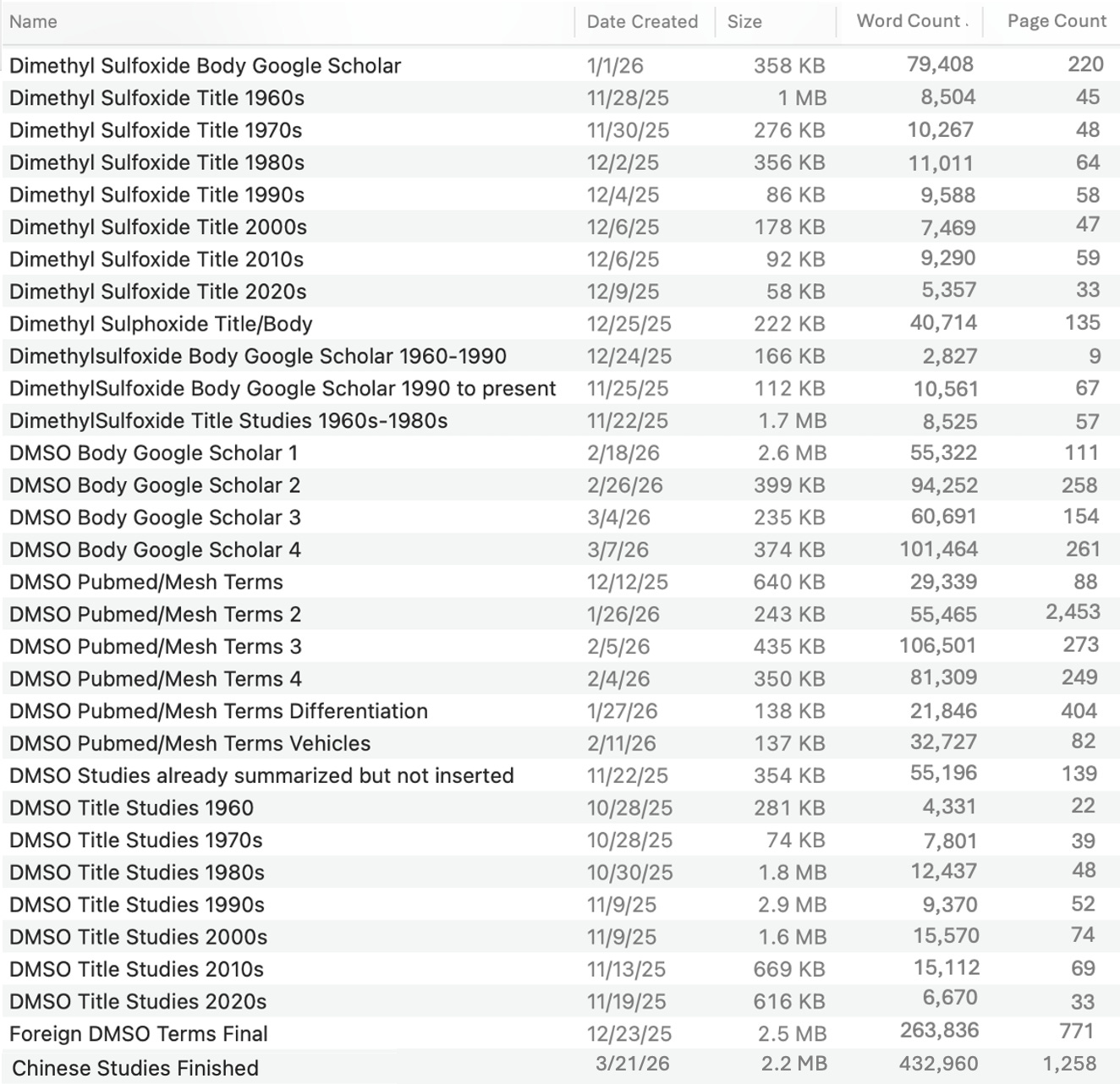
The goal is to build a comprehensive catalog of every medically relevant study ever conducted on DMSO—a therapy with an enormous and largely suppressed body of research.
Every applicable database. Every search term. Every result manually filtered to identify what was medically relevant and what wasn’t.
And it turns out, the scale of what this required was unlike almost anything previously attempted in independent medical research.

Some of the databases returned thousands of results. Some returned hundreds of thousands.
One file of Chinese studies alone ran to 432,960 words and 1,258 pages.
The complete research directory spans dozens of files, from a 1960s title study of 4,331 words to a Google Scholar body search containing over 100,000 words. Months of full-time work.
This comprehensive a catalog will likely never be assembled again. It was undertaken because the obligation to do it was too significant to ignore.
And that is what it looks like to actually achieve sufficient sensitivity in a research question.
Most published medical literature? It doesn’t even come close.
And yet most everyone trusts it without question.

Correctly engaging with medicine is itself a sensitivity-specificity problem.
Most medical interventions cause some harm, sometimes obvious, sometimes subtle.
But many have genuinely transformed humanity.
Conventional therapies, while not ideal, are often the best option available.
And with most conditions, multiple viable approaches exist, each with different tradeoffs.
The problem is that medicine rarely has an honest discussion about those tradeoffs, so suboptimal choices are routinely made, often with serious consequences.
That’s why the cautious default is so important: when a therapy carries real potential for harm, sometimes doing nothing is safer than pretending action is automatically better.

That cautious approach has real costs.
For many patients, going slowly isn’t free. Waiting too long for a treatment response can cause more harm than manageable adverse effects they might have tolerated.
But the opposite mistake can also be devastating. Move too quickly, and a protocol may never get the chance to work.
That’s why this philosophy fits non-emergent care better than emergencies.
In high-stakes medicine, doctors often have to use therapies with inherent harm because the alternative is letting someone die. Immense respect is owed to the doctors who operate where harm is a routine cost of saving lives.

Where the sensitivity/specificity framework becomes most difficult—and most consequential—is in cancer treatment, where the stakes on both ends are catastrophic.
A Midwestern Doctor’s approach navigating it can be found in the full article.
Sensitivity, Specificity, and the Art of Seeking Truth
Cancer is where this dilemma becomes almost impossible.
Many conventional therapies carry severe side effects and only modest efficacy. Others have made previously fatal diagnoses survivable—but at enormous quality-of-life cost. Natural therapies are sometimes independently effective. And if conventional treatment is delayed while exploring alternatives, the disease can progress beyond what any treatment can reach.
So what’s the best path forward?
If time exists, try natural options first. Look for underlying precipitating causes—estrogen dominance, micronutrient deficiencies, retained emotional trauma—that must be addressed alongside whatever protocol is chosen. Default to natural therapies supporting conventional treatment rather than replacing it.
UV blood irradiation is excellent for mitigating chemotherapy side effects. And some cancer patients have remarkable responses to repurposed drug protocols like ivermectin.

One example captures the precision principle.
Ivermectin can create neurological issues at higher oral doses. But in some cancer cases, the need for high oral dosing can be bypassed by mixing ivermectin into a paste and applying it directly to the skin above a tumor, where it frequently works much better than any oral protocol.
And that right there is the larger point.
The drug didn’t change. The targeting did.
And once a therapy is directed more precisely at the problem, lower doses can sometimes accomplish what broader dosing cannot.

Here’s the insight that changes everything:
A therapy doesn’t always need to be stronger. Sometimes it just needs to be aimed better.
When treatment is targeted to the real problem, lower doses can often produce the needed effect. That’s why weaker natural therapies can sometimes work in cases that seem to require stronger drugs.
The problem with higher doses is simple: they’re more likely to hit the target, but also more likely to hit things they were never meant to hit.
That is where many side effects come from.
Modern medicine often solves this by standardizing the protocol, pushing the desired effect, and accepting the patients who react badly as the cost of doing business.
And in the end, those patients are largely forgotten.

The greatest obstacle to any of this isn’t access to information.
It is the human tendency—trained from birth—to protect the ego at the cost of accuracy. To stay right rather than become more right. To commit to a position and defend it—regardless of what new evidence suggests.
We see this play out in front of us all the time. But we probably struggle to see it clearly when we’re doing it ourselves.
Publicly correcting the Sims narrative wasn’t comfortable. But it was done anyway, because a paradigm that prioritizes truth over being right requires someone modeling it—especially when it’s uncomfortable.
A false narrative, repeated without question for decades. Corrected. In public. And in writing.
That matters.

The DMSO series—the direct product of that months-long research project—will soon be available to subscribers of A Midwestern Doctor. It may be the most comprehensive review of DMSO’s medical applications ever compiled.
Subscribe so you don’t miss a thing.
Sensitivity, Specificity, and the Art of Seeking Truth
This isn’t about how the medical system is corrupt.
It’s about how hard it is to know anything accurately, and what it looks like to keep trying anyway, including when that means correcting yourself publicly.
Both things can be true.
Truth, in this framework, isn’t a destination you arrive at.
It’s a direction. A calibration you keep adjusting. A standard you keep failing to fully meet while moving gradually closer to it.
Most people, most institutions, most publications, and most fields have a stated commitment to accuracy and an unstated commitment to being right. The gap between those two things is where most of the damage gets done.
The Sims correction could have been quietly ignored as it already had been for years. Instead, it was written about—with the reasoning visible, the error named, and the mechanism explained.
That’s a different kind of credibility than the kind maintained by never admitting a mistake.
And that’s exactly what we need more of if we want to see change we’ve been waiting for.

Thanks for reading! This information was based on a report originally published by A Midwestern Doctor. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
Sensitivity, Specificity, and the Art of Seeking Truth
For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by A Midwestern Doctor:
How DMSO Heals the Spine and Reverses Paralysis
The Hidden Dangers of Hospital Births & How to Protect Your Family
What’s The Healthiest Water To Drink?
While you’re at it, give A Midwestern Doctor a follow. No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed. This is easily one of the most valuable accounts you’ll ever follow.

If you haven’t subscribed to this Substack yet, take a moment to read what some of the most powerful voices in the medical freedom/truth movement have to say:
“The Vigilant Fox has been putting in a lot of work to create a news platform that shares the stories we want to hear about and brings attention to the most important things to know about. If you want a daily newsfeed in alignment with our ...”
– A Midwestern Doctor, The Forgotten Side of Medicine
“The Vigilant Fox absolutely is on top of things. We must support our fighters, and the Fox is fighting with truth.”
– Tom Renz, Tom Renz’s Newsletter
“Excellent capture of key video presentations on evolving pandemic science.”
– Peter A. McCullough, MD, MPH, FOCAL POINTS (Courageous Discourse)

How about gender reassignment surgery, and imprisoning the parents who try and stop this abomination?
This is one of the most significant and profound editorials that I have read from all the substacks and gifted writers and investigators that I subscribe to. A sincere thanks for the hard work of verbalizing the phenomenom you describe in this analysis. I have a cousin in law that always was a gifted genius, became a pharmacist and then went to med school, became a trauma, thoracic surgeon, and went into private practice. Years later (2020) he almost quit speaking to me because I refused to get vaxxed, boosted and re-boosted and re-re boosted like his wife, daughter, mother in law, and other family members that lined up blindly to follow his orders. I also had a dear friend, fellow attorney, a woman who I have known and worked closely with for 20 years- a brilliant appellate attorney collaborated with me in numerous cases-- who became very distant and irritated when she learned that I had voted for "The Orange Man." Your explanation clears up the mystery and reveals a deep flaw of human nature that was exploited by the ultimate global psychopaths that controlledl the narrative and evil scientists (Fauci, et.al.), FDA, the W.H.O., CDC, etc.