
Why American Childbirth Costs the Most and Delivers the Least
A data-driven walk through the interventions, incentives, and blind spots shaping modern hospital birth, and what actually protects mothers and babies.


The following information is based on a report originally published by A Midwestern Doctor. Key details have been streamlined and editorialized for clarity and impact. Read the original report here.
A New York Times reporter did the unthinkable and exposed the “worst test in medicine” — the one that five decades of evidence says doesn’t work.
The research is damning: continuous fetal monitoring raises C-sections by 66% and instrumental deliveries by 16%, with no drop in infant deaths or disability.
It flags a problem that usually isn’t one, and doctors rush to cut the baby out.
It’s not just a false flag problem; it’s a money incentive. Sarah Kliff says the quiet part out loud:
“Nobody gets sued for doing the C-section. You only get sued for not doing the C-section.”
Doctors are so terrified of legal consequences that they’ll push unnecessary surgery on their patients, not for the baby’s health, but to protect their pocketbooks.
That’s how the cascade starts. In a hospital delivery, one intervention triggers the next. It’s like an avalanche that can’t be stopped.
Next thing you know, you’re recovering for weeks from a major surgery you never needed.
If someone you love is about to have their first baby, share this before they ever set foot in a labor and delivery unit.
A Midwestern Doctor investigated what hospitals don’t tell you about birth outcomes, and it only gets worse from here.
For most of human history, childbirth happened at home, guided by a midwife who had already done this hundreds of times.
Today it’s one of the most heavily monitored, medicated, and surgical events in modern medicine.
Something clearly changed, and it’s not women’s bodies. They’re just as capable today as they were thousands of years ago.
But today, most parents walk into a delivery room having no idea what may happen next—or why.

Somewhere along the way, birth stopped being treated as a normal life event and started being treated as a medical emergency waiting to happen.
The mother is placed on her back. Monitors go on her abdomen. An IV goes in her arm. Strangers poke and prod her in strange places. Unfamiliar people move in and out of the room on a schedule that has nothing to do with her body’s own timing.
Some of this saves lives. But some of it creates the very complications it’s meant to prevent.
Understanding the difference is important.

This information comes from the work of medical researcher A Midwestern Doctor. For all the sources and details, read the full report below.
The Hidden Dangers of Hospital Births & How to Protect Your Family

Doctors weren’t always part of childbirth. For most of early American history, midwives handled deliveries, and did so well enough to be paid in things like housing, land, and salary by their communities.
But that started to shift in the late 1700s, when it became fashionable for doctors to attend births in Europe. American doctors soon followed.
And once doctors were in the room, they needed a reason to stay there.

In 1895, a doctor opened Chicago’s first obstetric clinic. He trained doctors and nurses, developed real innovations like premature-infant incubators, and lowered childbirth mortality in the process.
But he also watched enough complications and deaths that he came to a sweeping conclusion: normal childbirth itself was dangerous, and needed to be medicalized to be survived.
By 1920, he was arguing that tools designed for genuinely difficult deliveries, like forceps and sedation heavy enough to make a woman partially unconscious, should be used routinely, even in births that weren’t complicated at all.
Other doctors at the time said this went too far. But it didn’t matter. He trained too many of the next generation of obstetricians for his approach not to win.

That was over a century ago.
The idea he planted never left.
The idea that birth is inherently pathologic, and only a doctor with tools can save a mother and baby from it.
The idea that approaching birth from a different perspective is downright dangerous.

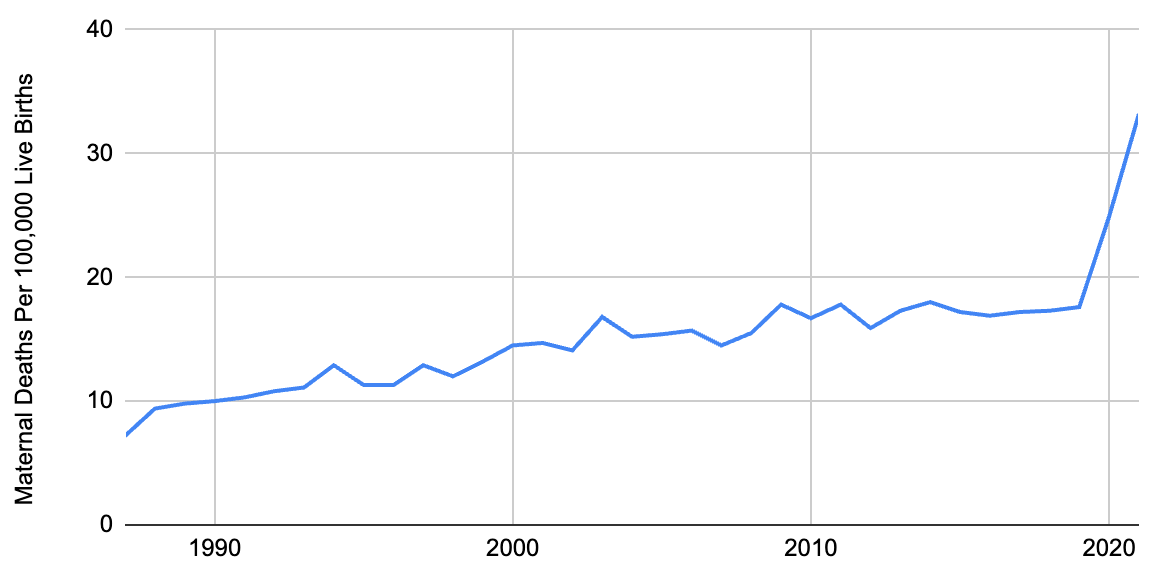
Here’s what makes that idea hard to defend. The U.S. maternal death rate was actually at its highest between 1900 and 1930, the exact period when standardized, invasive delivery practices took hold.
It took decades of further mistakes before outcomes started to improve.
And even now, over a century later, the U.S. still ranks last among wealthy nations in both infant and maternal mortality, despite spending at least $111 billion a year on childbirth, roughly twice what most high-income countries spend.
That history explains the mindset that still runs the delivery room today.
But some of what happens today goes even further than doctors of that era imagined.
Let’s start with the ultrasound. Every doctor is trained that it is simply “safe,” full stop, with the only caveat being that image quality is operator-dependent.
The literature tells a more complicated story. In a dose-dependent manner, animal studies have linked ultrasound exposure to genetic damage, cell death, organ damage, and behavioral impairment.
The most striking data comes from 40 Chinese studies conducted in the 1980s, where women already scheduled for abortion were randomized to receive an ultrasound beforehand, after which the fetus was dissected. Across those studies, ultrasound consistently produced measurable damage to intracellular structures and organs.
That’s not a fringe finding buried in some obscure journal. It’s a body of dissection-level evidence that never made it into the safety conversation most parents hear.
Today, many women receive multiple ultrasounds throughout their pregnancy without so much as a second thought about the safety.

In 1991 and 1992, the FDA raised the allowable output of ultrasound machines 15.7-fold, at manufacturer request, because higher power produced sharper images.
This happened despite existing literature already showing harm at the lower doses. The now common doppler ultrasound outputs even more than standard ones.
A safety limit didn’t move because new safety data justified it. It moved because the pictures looked better.

That 1991–92 power increase lines up closely with the years autism diagnoses began climbing, a rise usually attributed entirely to other causes. This doesn’t prove anything, but it raises some important questions worth considering.
And these are exactly the kinds of questions a genuinely safety-minded system would have investigated decades ago instead of leaving to a chart nobody in mainstream medicine has been willing to publish.

This doesn’t mean every ultrasound is a mistake. Some pregnancies genuinely need them, and a brief scan near the end of pregnancy can catch real emergencies, like an umbilical cord in the wrong position, that some birth plans just couldn’t safely handle.
The distinctions that can matter here are early versus late and routine versus necessary. Early scans, done when a fetus is most sensitive, add the least clinical value and the most theoretical risk. A late, brief scan for an actual need closer to delivery is a different calculation.

Ultrasound isn’t the only “routine” step worth questioning before you walk into a delivery room. A Midwestern Doctor full piece lays out the specific alternatives worth knowing about, and when a scan is actually worth it.
The Hidden Dangers of Hospital Births & How to Protect Your Family
Here’s what a standard hospital delivery actually looks like once labor starts.
The mother is placed on her back with her legs elevated, and she’s hooked to continuous fetal monitoring. If labor moves too slowly by the hospital’s clock, she’s given synthetic oxytocin to speed contractions and may have her water broken to “speed things up.”
Her pain is managed with an epidural. Pain is expected if you’re trying to hurry things along against mom’s body’s clock.
If the baby doesn’t descend fast enough, forceps or a vacuum come next.
And if none of that works, it becomes a C-section.
Each step may defensible on its own. But stacked together, they function less like individual medical decisions and more like a sequence. A sequence that completely ignores what mom and baby are doing.

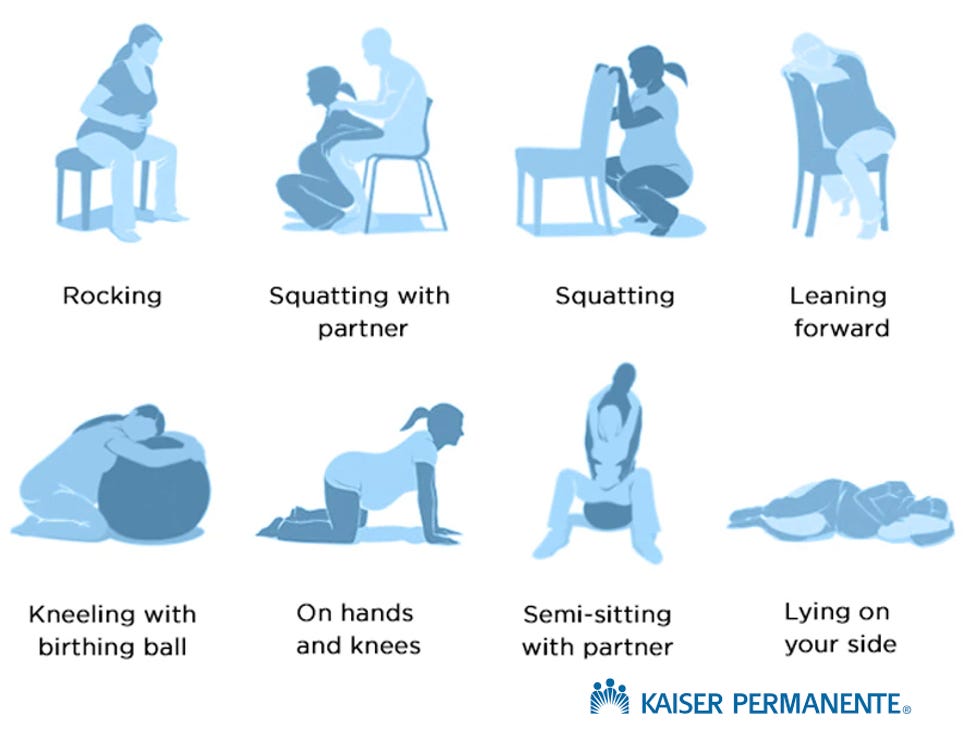
When it comes to the actual birth, let’s start with posture. In most hospital births, 68% of mothers deliver flat on their backs, and another 23% deliver reclined.
Compare that to home births, where mothers choose their position freely. Only 8% choose to lie flat.
That’s a huge gap and there’s a big reason for it. Lying down closes the pelvis and compresses a major vein carrying blood back to the heart, reducing blood flow to the baby.
A 2017 Cochrane-adjacent review found upright delivery reduced abnormal fetal heart rates, sped up labor, and cut the need for forceps or episiotomies.
And yet 68% of mothers deliver on their backs in hospitals.
Position is just the entry point.
Once labor is underway inside a hospital, the interventions don’t happen in isolation. Each one tends to make the next one more likely.

Continuous fetal heart monitoring is treated as a safety cornerstone in nearly every hospital birth. But a Cochrane review comparing it to periodic stethoscope checks found it doesn’t reduce infant death or disability.
What it does do is increase the odds of a C-section by 66% and an instrumental delivery by 16%, because abnormal readings push doctors toward intervention even when the baby is fine.

Then there’s pitocin, synthetic oxytocin used to speed up labor that’s deemed too slow—usually according to the hospital’s clock.
Given at too high a dose, it produces contractions strong and frequent enough to increase anal sphincter tears by roughly 80%, raise the risk of postpartum hemorrhage, and compress the baby’s blood supply enough to trigger the very heart rate abnormalities that lead to a C-section.
One intervention manufactures the justification for the next one.

Roughly 70–75% of hospital births use an epidural. It’s genuinely helpful for pain, especially once other interventions have made labor harder to tolerate.
But it comes with real trade-offs.
In one study of 439 women, 41.9% had a measurable systemic reaction, including severe drops in blood pressure in over a third. That blood pressure drop worsened fetal heart rate in over 11% of cases.
Evidence on whether epidurals raise C-section risk is mixed on their own, but combined with pitocin, one study found the risk climbed sixfold.
Plenty of mothers need and benefit from an epidural. But it is important that they know what they’re trading before they’re mid-labor and being asked to decide in sixty seconds or less.

All of it tends to funnel toward the same outcome.
Nearly a third of American births now end in a C-section.
That was 32.4% of births in 2024.
But the WHO estimates roughly 10% of births actually require one to prevent death.
So why is the number so high?

A C-section is major abdominal surgery, and it carries the risks that come with one: a 4–6 week recovery, a global infection rate above 5%, and a real chance of accidental injury during a procedure sometimes performed under real time pressure.
There are also risks specific to the surgery itself.
Two C-sections make a woman roughly 14 times more likely to have a dangerous placenta attachment in a future pregnancy.
A weakened uterine scar can rupture during a later labor, which is part of why one C-section often locks a woman into needing every subsequent delivery to be surgical too.

Beyond the surgery, bypassing the vaginal birth process itself disrupts something less obvious: the transfer of bacteria that colonizes a newborn’s gut.
That disruption has been linked to a measurable rise in childhood asthma, hay fever, and a cluster of autoimmune conditions including celiac disease and inflammatory bowel disease.
That’s a really big deal.

The most striking data goes much further than the immune system.
Children born by C-section show a 23–26% higher rate of autism and a 15–16% higher rate of ADHD. A large study found the autism signal was strongly correlated with whether the mother received general anesthesia during the procedure, not the surgery alone.
Imaging studies back this up structurally. One MRI study of 306 children found C-section birth associated with reduced brain white matter and weaker functional neural connectivity. A 2017 study published in Nature found C-section children performed measurably lower on standardized testing years later, even after controlling for other variables.
That’s not a small footnote. That’s a signal running through immune function, cognition, and behavior, tied to a procedure performed on nearly a third of American births.
This is absolutely something worth looking into.

Every day, C-sections save lives in exactly the situations that the surgery was designed for.
But at the same time, women elect to have scheduled C-sections because it fits their or their doctor’s calendar better.
Both things can be true: essential in the moments that call for them, and dramatically overused in the moments that don’t.

Here’s what actually moves the needle in the other direction, and neither one requires new technology.
Skin-to-skin contact immediately after birth has been shown to cut NICU admissions for low blood sugar by half, improve a newborn’s gut microbiome, and reduce postpartum depression and PTSD in mothers, including after a C-section. And if needed, that contact can come from dad or even a twin.
Delayed cord clamping, simply waiting before cutting the umbilical cord, increases a baby’s blood volume by up to a third, cuts brain bleeds in premature infants by roughly 60% in one study, and reduces a serious intestinal condition called necrotizing enterocolitis by 41%.
Only about half of U.S. hospital births currently practice delayed cord clamping.
One more variable outperforms almost everything else on this list, and it isn’t a medical procedure at all.
A Cochrane review found continuous labor support from a doula was associated with a 25% lower chance of a C-section, labors that were 41 minutes shorter on average, an 11.7% drop in epidural use, and a 38% lower chance of a low five-minute Apgar score for the baby.
One study even found that training a friend for two hours produced many of the same benefits as a professional doula.
The support itself is what matters.
And if in a hospital environment, that support can step in and help a mother avoid many of the interventions we’ve discussed here if that’s what she wants.

The full article from A Midwestern Doctor details exactly how to mitigate C-section complications after the fact, when cord blood banking makes sense versus delayed clamping, and specific methods for correcting a breech baby before delivery—because it is possible.
The Hidden Dangers of Hospital Births & How to Protect Your Family
The pattern isn’t random.
A hospital vaginal birth runs $13,000–$18,000. A C-section runs $25,000–$30,000—sometimes far more with complications.
A home birth with full midwife care costs a fraction of a hospital birth.
Obstetric units are often understaffed enough that deliveries have to be sequenced and accelerated so they don’t collide. Add liability risk for any doctor who deviates from standard protocol, and the system is quietly built to reward speed and intervention over patience.
That’s not a conspiracy. It’s an incentive structure. And incentive structures produce exactly the outcomes you’d expect them to.

If you or someone you know is pregnant, don’t miss the full article.
A Midwestern Doctor shares the best setup for where to give birth, preferred alternatives to routine ultrasound, safe anesthetic options, and a full breakdown of preventing and correcting problems like preeclampsia, edema, and miscarriage risk before they become emergencies.
The Hidden Dangers of Hospital Births & How to Protect Your Family
None of this is really about hospitals versus home, or intervention versus none. It’s about who gets to make the decision, and whether they’re making it with real information or with whatever a rushed, liability-driven system hands them in the moment.
Birth was never supposed to be an assembly line.
It was supposed to be one of the most significant events a family ever moves through, one that deserves patience—not a protocol built around how many other deliveries are happening down the hall or when a doctor wants to go golfing.
Somewhere in the last century, that got lost. Finding it again starts with knowing what actually happened, and what’s actually true.

Thanks for reading! This information was based on a report originally published by A Midwestern Doctor. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
The Hidden Dangers of Hospital Births & How to Protect Your Family
For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by A Midwestern Doctor:
How DMSO Heals the Spine and Reverses Paralysis
What They Don’t Tell You About C-Sections
What’s The Healthiest Water To Drink?

While you’re at it, give A Midwestern Doctor a follow. No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed. This is easily one of the most valuable accounts you’ll ever follow.
If you haven’t subscribed to this Substack yet, take a moment to read what some of the most powerful voices in the medical freedom/truth movement have to say:
“The Vigilant Fox has been putting in a lot of work to create a news platform that shares the stories we want to hear about and brings attention to the most important things to know about. If you want a daily newsfeed in alignment with our ...”
– A Midwestern Doctor, The Forgotten Side of Medicine
“The Vigilant Fox absolutely is on top of things. We must support our fighters, and the Fox is fighting with truth.”
– Tom Renz, Tom Renz’s Newsletter
“Excellent capture of key video presentations on evolving pandemic science.”
– Peter A. McCullough, MD, MPH, FOCAL POINTS (Courageous Discourse)

We already know they want us dead but, we’ll reckon they would come after our offspring 🥲 these Ppl are sick evil wether their aware or not just sayin it
"Nearly a third of American births now end in a C-section. That was 32.4% of births in 2024."
"Children born by C-section show a 23–26% higher rate of autism and a 15–16% higher rate of ADHD."
ADHD,which is associated with C-section, is associated with a higher average risk of psychopathy and antisocial personality disorder and later antisocial behaviour than the general population.
Birth by C-section is weakly associated with a lower general cognitive ability in young adult males.
Great!!! America arguably already has more low iQ psychopaths than other developed Western and even Communist and Islamic countries!!! Churning out even more is just what's needed. What could possibly go wrong???