
What Happens When the Body Doesn’t Get Enough Salt?
Low-salt diets are prescribed by doctors to millions of people a year—yet few are warned about the dangers that come with such a diet.


The following information is based on a report originally published by A Midwestern Doctor. Key details have been streamlined and editorialized for clarity and impact. Read the original report here.
The world’s #1 biohacker does something every morning that most doctors would freak out about.
He takes SALT with his morning water.
We’re not talking about table salt here.
The process salts you see today are stripped of the trace minerals you need.
Instead, Gary Brecka uses Baja Gold Sea Salt.
“That’s probably the best salt that you can put in the human body because it has all 91 trace minerals,” Brecka says.
It’s also tested to make sure it’s free of microplastics and glyphosates.
For years, science has waged a war against salt, calling it the cause of high blood pressure and heart disease.
Low-salt diets are prescribed by doctors to millions of people a year—yet few are warned about what happens when the body doesn’t get enough salt.
For half a century, we’ve been told something so often it feels completely unnecessary to question it:
Salt raises blood pressure.
High blood pressure causes heart disease.
Therefore, salt is dangerous.
It’s simple. Linear. Clean.
But it might be one of the most oversimplified stories in modern medicine.
And if we’ve been led to believe something is unquestionable simply because we’ve heard it repeated so many times… well that’s a clear indication that we should probably start questioning it.

The war on salt didn’t begin with overwhelming data.
It began in 1977, when a Senate committee recommended sodium restriction despite evidence not clearly supporting it.
From that moment forward, a hypothesis hardened into doctrine. And doctrine rarely retreats quietly.
Over the next few decades, something else happened.
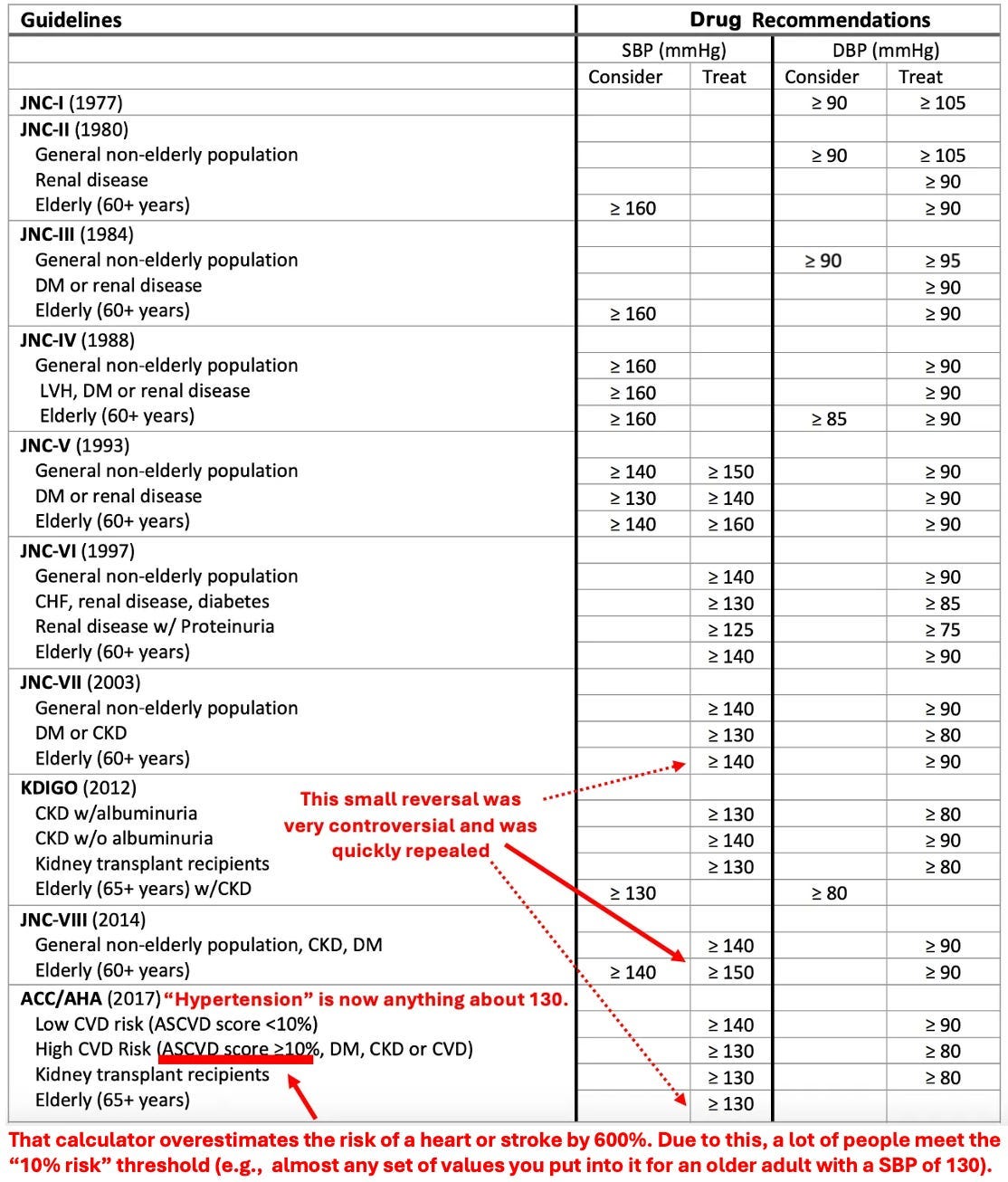
Blood pressure thresholds were gradually lowered. The definition of “normal” narrowed. More people became hypertensive overnight—not because physiology changed, but because the number did.
And once a number becomes a treatment target, an industry grows around it.
Here’s where the salt story starts to fracture.
The most detailed review of sodium restriction found that drastic salt reduction typically results in less than a 1% reduction in blood pressure.
Less than 1%.
Less.
Than.
One.
Percent.
That’s the measurable effect that justified telling millions to eliminate a basic mineral from their diet.

The full report from A Midwestern Doctor goes much deeper into the research behind the <1% blood pressure effect and how that statistic became public policy.
It includes data rarely discussed in mainstream guidelines. Don’t miss it.
What They Never Tell Us About Salt

Now consider this:
Hospitalized patients routinely receive IV 0.9% sodium chloride. In many cases, they are given amounts equal to ten times the recommended daily sodium intake.
Wait… what?!
If salt were a direct and powerful driver of hypertension, we would expect dramatic spikes.
Instead, blood pressure often barely moves.

This doesn’t mean salt has no effect.
Some individuals are salt-sensitive. Certain ethnicities may respond differently. Edge cases exist.
But public health messaging treated the edge case as the default condition.
It’s not.

And then there’s hyponatremia.
Low sodium isn’t rare. It’s one of the most common electrolyte abnormalities seen in hospitals.
Between 15% and 20% of hospitalized patients arrive with low sodium levels.
We’re not talking about fringe physiology. We’re talking about everyday admissions.

It gets even more uncomfortable.
The sodium targets many people are encouraged to follow are associated with a 25% increase in mortality risk.
Low dietary sodium intake has also been linked to a 34% increase in cardiovascular disease and death.
Low sodium = increase in disease and death.
And that’s not marginal. That’s structural.

The full breakdown in A Midwestern Doctor’s report walks through the hyponatremia data, the 25% mortality increase, and why low sodium is so common in hospitals.
It’s a side of the salt story most people have never seen.
What They Never Tell Us About Salt
Salt restriction in hypertensive patients made them 9.9 times more likely to develop hyponatremia.
And many common medications—especially SSRIs—increase the risk even further, by over threefold.
So while we warn people about “too much salt,” we quietly increase the risk of too little.

What does low sodium actually feel like?
Fatigue.
Confusion.
Difficulty concentrating.
Lightheadedness.
Falls.
These aren’t exotic symptoms. They’re among the most common reasons elderly patients land in emergency rooms.

When sodium drops rapidly, cardiac output falls. Blood pressure collapses. The heart compensates by racing.
Clinically, it can resemble traumatic shock.
Yet culturally, low salt is framed as inherently virtuous.

Some patients with chronic fatigue, POTS, and orthostatic intolerance improve dramatically when dietary sodium is increased.
Because sometimes low blood pressure—not high blood pressure—is the real issue.
The body doesn’t worship low numbers. It worships balance.

You may have noticed that biology doesn’t operate in straight lines.
It operates in curves.
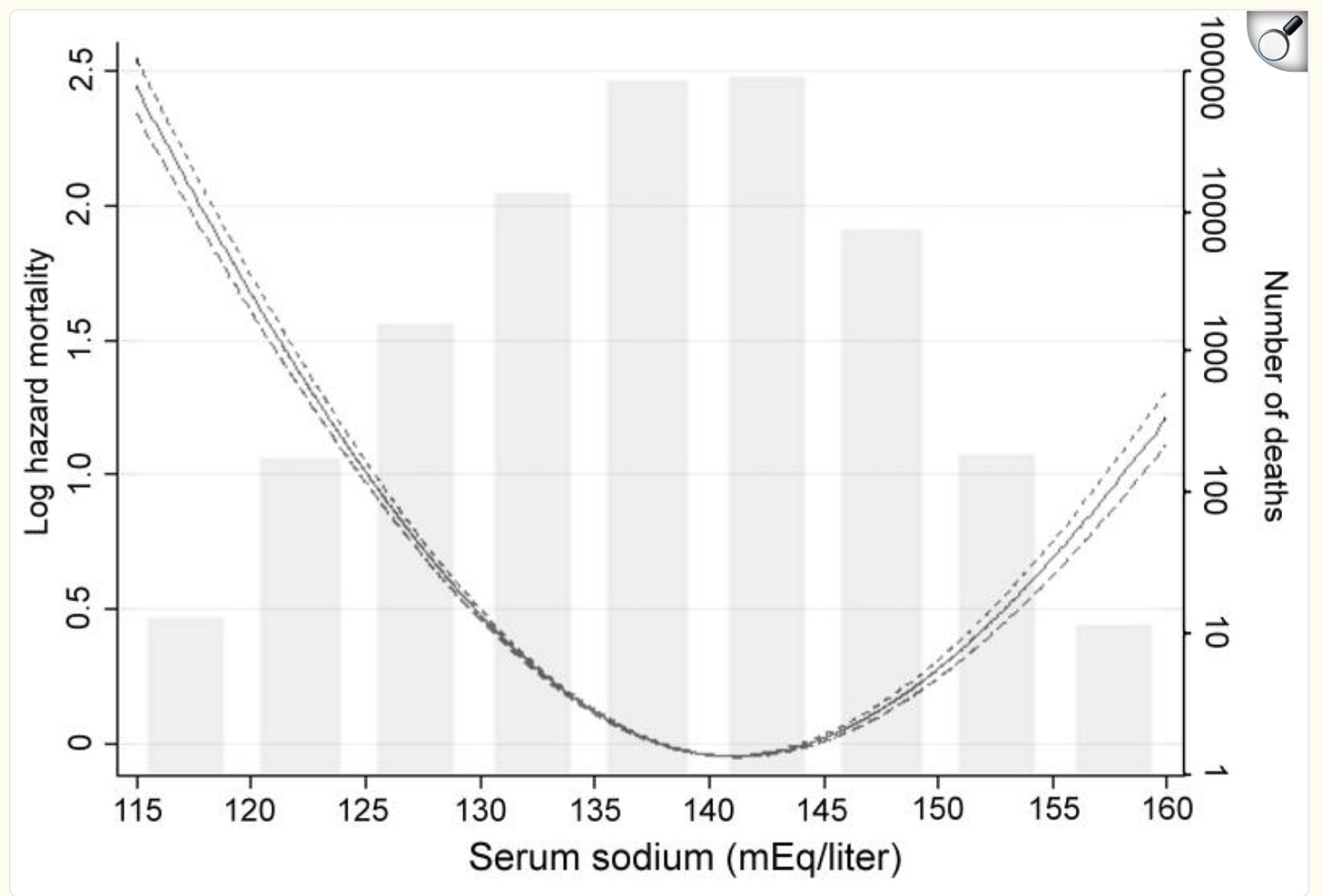
Both very high and very low sodium levels are associated with increased mortality. The relationship is U-shaped.
Extremes are dangerous. Moderation is protective.
In patients with chronic kidney disease and heart failure, mortality risk was lowest in the mid-range of sodium levels.
Too low increased risk. Too high increased risk.
The safest zone was not at one extreme—but in the middle.
Ideal salt intake isn’t one size fits all.
The full report from A Midwestern Doctor explores the U-shaped mortality curve in detail and why biology doesn’t operate in straight lines.
It connects the physiology, the data, and the policy decisions behind it.
What They Never Tell Us About Salt
This is where linear thinking breaks down.
Medicine often sees a harmful high number and assumes lowering it indefinitely must be beneficial.
But once blood pressure—or sodium—drops too low, risk reverses direction.
And that reversal is rarely discussed.

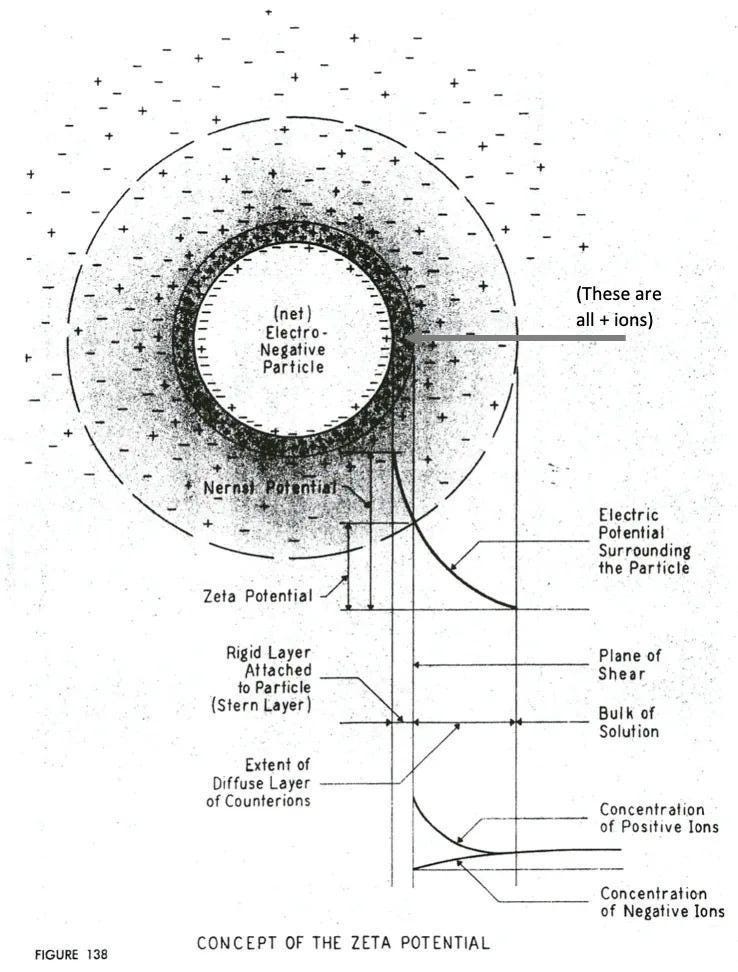
There’s also a deeper physiologic layer at play. It’s called zeta potential.
This describes the electrical stability of particles suspended in fluids—like blood cells.
When electrical balance is disrupted, particles clump. Circulation becomes inefficient. Congestion increases.
Zeta potential also follows a U-shaped curve.
Sodium plays a role in achieving balance. Too little can impair physiologic stability. Too much—especially in refined form—can as well.
This may explain something clinicians observe but rarely frame correctly:
IV saline frequently improves hospitalized patients quickly.
It’s labeled “rehydration.” But in many cases, it may simply be correcting sodium depletion that destabilized circulation.
Maybe you’ve had this experience yourself—feeling relief with the IV drip, regardless of what you’ve hospitalized for.

Modern diets really complicate the salt story.
Keto increases sodium excretion. Processed foods alter mineral ratios. Potassium intake has fallen as whole foods were replaced with refined products.
It’s not just sodium. It’s sodium relative to potassium.
It’s all about balance—again!

There’s also the distinction between refined and natural salt.
Refined salt is stripped of trace minerals. Anti-caking agents are added. Industrial processing may involve chemicals like sodium carbonate or sodium hydroxide.
That’s obviously not how salt exists in nature.

Many of the worst “salt overload” experiences people report occur after eating processed foods—not after consuming natural salts.
That distinction matters.
When you isolate a mineral from its natural context, physiology often responds differently.

Meanwhile, blood pressure targets continued to narrow.
Millions were medicated to levels that reduce organ perfusion, increase fall risk, worsen kidney function, and impair cognition.
Sometimes high blood pressure is compensatory—not causal.

When medicine fails to address root causes, it often chooses a scapegoat.
The sun.
Eggs.
Saturated fat.
Salt.
Simple villains make complex systems easier to manage.

The takeaway here is that salt isn’t harmless, but neither is sodium depletion.
The real question isn’t whether or not salt affects health, it’s whether we built a 50-year policy on a linear model—when human biology has always operated in curves.
And all signs point to the failed linear model.
Today seems like a good day to starting shifting your relationship with salt!

Thanks for reading! This information was based on a report originally published by A Midwestern Doctor. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
What They Never Tell Us About Salt
For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by A Midwestern Doctor:
Unmasking The Great Blood Pressure Scam
The FDA’s 50-Year War on the Safest Painkiller Ever Discovered
What’s The Healthiest Water To Drink?

While you’re at it, give A Midwestern Doctor a follow. No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed. This is easily one of the most valuable accounts you’ll ever follow.
If you haven’t subscribed to this Substack yet, take a moment to read what some of the most powerful voices in the medical freedom/truth movement have to say:
“The Vigilant Fox has been putting in a lot of work to create a news platform that shares the stories we want to hear about and brings attention to the most important things to know about.”
– A Midwestern Doctor, The Forgotten Side of Medicine
“The Vigilant Fox absolutely is on top of things. We must support our fighters, and the Fox is fighting with truth.”
– Tom Renz, Tom Renz’s Newsletter
“Excellent capture of key video presentations on evolving pandemic science.”
– Peter A. McCullough, MD, MPH, FOCAL POINTS (Courageous Discourse)

I was already heavy into fitness as a teenager in the mid 1960s. I read from the sources I trusted way back then to not worry about salt, the body excretes excess unless you have an unusual condition, eggs are the most perfect food, dietary cholesterol has minimal impact on blood cholesterol, eat butter not margarine. All facts shown by real science by the 60s. I'm glad I learned early to spot how badly the "experts" lie, and they are not about real science at all. I was immune to the COVID bs thank God.
I had a slightly different problem when I nearly collapsed at home and my wife rushed me to the ER. I started to feel better fairly quickly as they were running me through all kinds of tests but found nothing wrong. I am sure it was just the salinated water they injected as soon as I arrived. The prior month I had cut my coffee consumption in half but failed to drink water to replace it.
Whether it was low sodium or low water, I didn’t know and neither did they as they told me they found nothing and sent me home. On returning home, I thought about it and figured it out myself!