
The Dark Side of Antidepressants That Never Makes TV News
If you or someone you love is taking them, you might want to read this.


The following information is based on a report originally published by A Midwestern Doctor. Key details have been streamlined and editorialized for clarity and impact. Read the original report here.
Surprise, surprise: it turns out antidepressants may have been propped up by deeply flawed science.
“Most clinical drug trials have found the effectiveness of antidepressants is ON PAR with placebo,” wrote Dr. Joseph Mercola.
On the other hand:
“Large-scale meta-analyses show that physical exercise is the most effective remedy — about 1.5 times more effective than antidepressants — for depression.”
You probably never heard that on TV because in 1996, Bill Clinton signed the Telecommunications Act, which allowed Big Pharma to buy off the news.
Here’s what else they’re not telling you about antidepressants. If you or someone you love is taking them, you might want to read to this.
For decades, antidepressants have been sold as a simple fix for depression. Low serotonin. Take a pill. Problem solved.
But what if that story was never accurate? What if the real picture is far more complicated? And far more disturbing?
SSRIs were marketed as a clean fix for a “chemical imbalance.” But internal trial data shows something far darker—suicide signals, psychotic reactions, violent behavior.
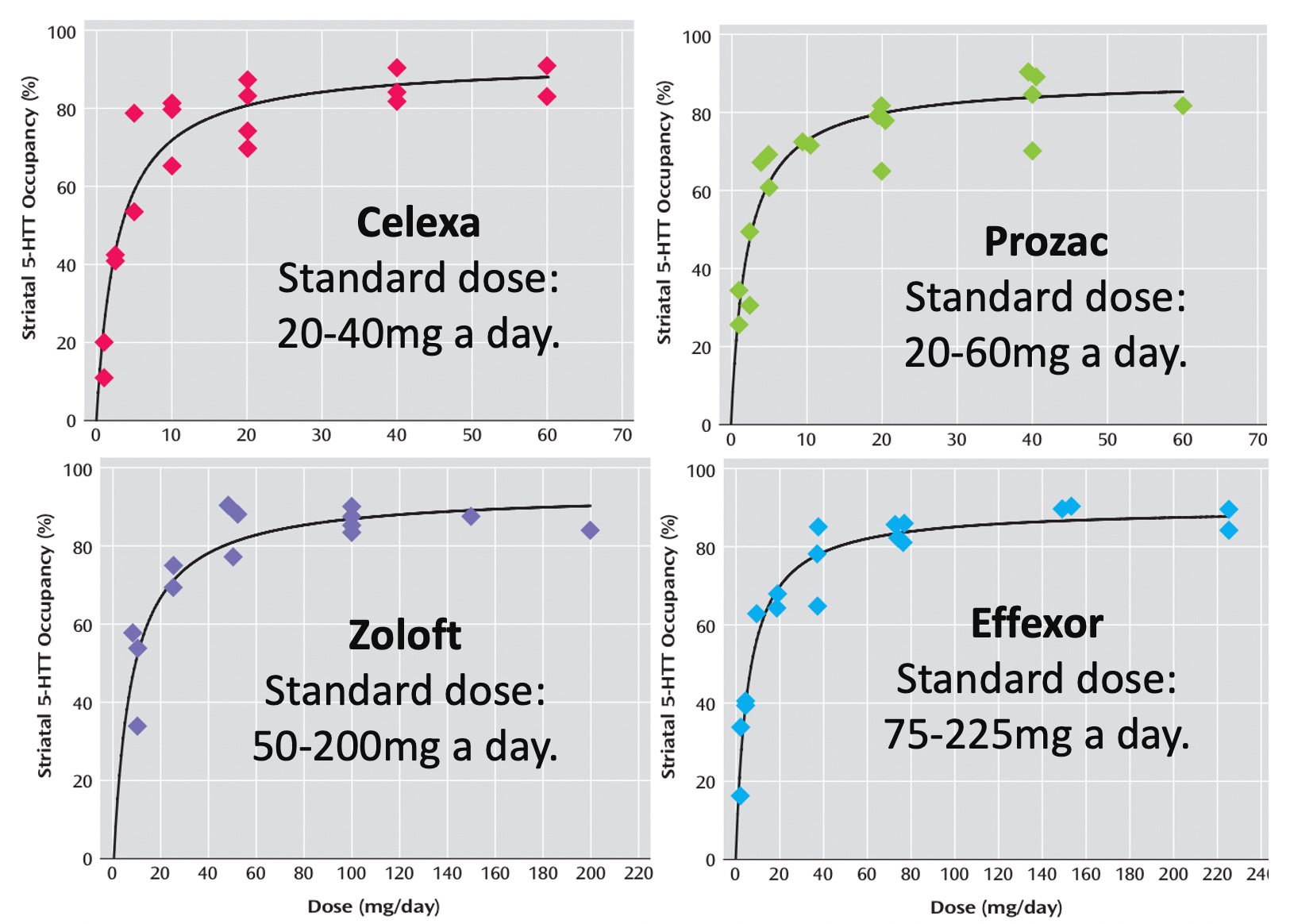
The FDA received 39,000 complaints in the first nine years after Prozac hit the market.
That wasn’t fringe. That was an early warning.
Millions of Americans are on SSRIs right now.
Many were told these drugs are safe, effective, and non-addictive. Many were never warned about emotional numbness, sexual dysfunction, manic episodes, or brutal withdrawals.
If even a fraction of the claims in this report from A Midwestern Doctor are true, we’re looking at one of the biggest medical blind spots of our time.

The violent behavior issue wasn’t discovered decades later after these drugs hit the market.
It showed up in clinical trials.
Families later uncovered documents during lawsuits indicating the risk was known—and minimized.
A 1991 FDA hearing even addressed antidepressant-linked suicide and violence.
That was 35 years ago!
This information comes from the work of medical researcher A Midwestern Doctor. For all the sources and details, read the full report below.
What Everyone Needs to Know About Antidepressants

The extreme cases grab headlines.
But toxicology follows a bell curve.
When unmistakable severe reactions appear, it usually means far more moderate injuries are happening quietly underneath.
The psychotic violence may just be the visible tip.

Clinical trials are supposed to tell us the truth.
But when you look closely at antidepressant trials, something odd appears.
High dropout rates.
Placebo groups that look surprisingly similar to drug groups.
Patients stopping the medication at alarming rates.
In one review, 77% more people stopped Paxil due to side effects than placebo. In another dataset, more than half of patients quit SSRIs within four months.
If a medication designed to make people feel better causes this many to walk away, what does that tell you?

A study of 7,525 patients found 56% stopped their SSRI within four months.
An international survey found 44% permanently quit psychiatric meds due to side effects.
81.5% said they weren’t sure their antidepressant was even necessary.
That’s not confidence.

Here’s where it gets darker.
In trials involving healthy volunteers with no history of depression, some participants reportedly became suicidal after starting SSRIs.
Not depressed before.
Not unstable before.
Then suddenly overwhelmed with suicidal ideation after.
Even critics who dismiss anecdotal stories struggle to explain why healthy individuals would spiral like that.
The standard explanation is that the drugs “unmask” something already there.
But what if, in some cases, the drug is the trigger?

In a survey of 1,829 antidepressant users in New Zealand:
• 62% reported sexual difficulties
• 60% felt emotionally numb
• 52% felt “not like themselves”
Nearly 40% experienced suicidal ideation.
Those aren’t rare events.

The most common side effect isn’t violence. It’s emotional anesthesia.
Forty to sixty percent of users in some studies report emotional blunting.
They don’t feel as low, but they also don’t feel joy.
Colors seem less vivid. Relationships feel distant. Motivation fades.
People describe it as watching their own life through glass. Psychiatry calls it emotional blunting. Others call it something closer to sedation of the soul.
Regardless of the name, it sounds like a tragedy.

The most devastating thing isn’t even about suicide. It’s about sex.
More than half of people taking SSRIs develop some form of sexual dysfunction. Some report permanent loss of sensation years later. And almost no doctors warn patients.
What Everyone Needs to Know About Antidepressants
In one Spanish study, nearly 60% of patients experienced significant sexual disturbances after starting SSRIs.
Decreased libido.
Delayed orgasm.
Complete inability to climax.
For some, the problem persisted long after the drug was stopped. 40% considered the dysfunction unacceptable.
Imagine taking a pill to feel better, only to lose one of the most fundamental parts of human intimacy.
How many were warned before their first prescription?

Some patients report that the dysfunction never fully reverses.
This condition has a name now, Post-SSRI Sexual Dysfunction, or PSSD.
People describe numb genitals, emotional detachment, loss of romantic capacity.
Doctors often dismiss it as psychological.
Yet more and more patients tell identical stories.
When thousands of strangers describe the same pattern independently, at what point do we stop calling it coincidence?

This is only scratching the surface.
A Midwestern Doctor’s full report goes much deeper into the data, the mechanisms, and the patient stories.
If you think you understand antidepressants, you probably don’t.
Read the full breakdown:
What Everyone Needs to Know About Antidepressants
SSRIs are stimulatory drugs.
Label warnings include anxiety, agitation, hostility, impulsivity, akathisia, hypomania, mania.
Those overlap heavily with stimulant drug effects. In some individuals, that stimulation escalates dangerously.

SSRIs are associated with manic switches.
Patients treated for depression sometimes convert to bipolar disorder after exposure to antidepressants.
Some datasets suggest the conversion rate is several times higher among those on antidepressants compared to those who never took them. hmm.
The explanation given is that the drugs simply revealed latent bipolar disorder.
But consider the timing… In 1955, bipolar disability was rare. Today, it affects between 1 in 20 and 1 in 50 people.
What changed?

What if some “bipolar disorder” isn’t unmasked—but induced?
60% of bipolar patients in one survey reported symptoms began after SSRI treatment.
That changes the risk calculation entirely.
What Everyone Needs to Know About Antidepressants
When mania hits, it can be explosive.
Agitation.
Impulsivity.
Racing thoughts.
And in severe cases, psychosis.
There are documented hospital admissions where patients starting SSRIs rapidly developed mania or psychotic symptoms.
Some heard voices telling them to harm themselves.
The official line says the medication treats mood disorders.
Yet in some cases, it appears to create them.

Pregnancy adds another layer.
SSRIs are often prescribed to pregnant women struggling with mood changes. Mood changes are common during and after pregnancy due to shifts in hormones and other stressors.
But studies cited show increased risks of premature birth and septal heart defects.
In one large Danish study, the risk of septal defects increased from 0.5% to 0.9% with one SSRI, and over 2% with multiple.
Persistent pulmonary hypertension in newborns has also been linked in some research.
Even small percentage increases matter when millions are exposed.
And if that’s not concerning enough, here’s the most brutal part.
Withdrawal.
A recent meta-analysis cited in the report found a staggering 56% of people stopping SSRIs experienced withdrawal symptoms.
Nearly half described them as severe.
These are not mild mood dips. People report electric shock sensations known as brain zaps, crushing anxiety surges, derealization, muscle spasms, suicidal thoughts.
Some last weeks. Some last months.

Here’s the catch: When patients show up in distress after stopping, they are often told it is a relapse.
Not withdrawal. Relapse.
So they’re put back on the drug.
The same drug that may have caused the dependency in the first place.
That cycle keeps many trapped—for years.

Tapering off safely can take an astonishing amount of time.
Because of how SSRIs bind to receptors in the brain, reducing the dose requires progressively smaller cuts.
Some patients reduce by 10% per month. That can mean years to fully come off.
In some cases, it takes longer to quit the drug than the time spent taking the prescribed dose.
Does that sound non-addictive?
Why does tapering take years?
Because these drugs don’t just alter mood—they alter receptor density and neural wiring.
And rewiring back can be slow, chaotic, and brutal.
What Everyone Needs to Know About Antidepressants
There’s an entire online community devoted to surviving antidepressants.
Thousands of detailed case histories.
People sharing taper schedules, coping strategies, setbacks.
When that many independent stories converge, it suggests a systemic issue, not isolated bad luck.

So if the standard model of depression is incomplete, what then?
There’s growing discussion that depression isn’t one disease.
Metabolic research has identified subtypes involving:
Low cerebral folate.
Copper overload.
Amino acid abnormalities.
Tetrahydrobiopterin deficiencies.
Treating the wrong subtype with a blanket SSRI may not just fail—it may harm.
There’s growing evidence linking inflammation and depression.
Chronic infections.
Mold exposure.
Lyme disease.
Long COVID.
When inflammation improves, mood often improves.
The brain is not isolated from the body. It reflects what’s happening systemically.
A serotonin reuptake inhibitor doesn’t address all of that. Treating depression as a pure serotonin imbalance may miss the root cause entirely.
Hormones also matter.
Low testosterone in men can manifest as fatigue and depression.
Progesterone shifts in women can influence mood profoundly.
Thyroid dysfunction can mimic major depressive disorder.
If the underlying issue is hormonal, an SSRI may dull symptoms without fixing the imbalance.
That is symptom management, not restoration.

Then there’s trauma.
Adverse childhood experiences are strongly linked to adult depression.
The nervous system adapts to stress and sometimes gets stuck in defensive mode.
In that state, numbing symptoms with medication can provide short-term relief. But without resolving the trauma, the core wound remains.
No pill can fully substitute for safety, connection, and healing.
Some clinicians are exploring psychedelic-assisted psychotherapy, including ketamine and psilocybin, to address treatment-resistant depression.
These approaches aim to increase neuroplasticity and help patients process trauma.
The early data is promising, though not without risks.
The key difference is intention. Rather than suppressing symptoms indefinitely, the goal is transformation.
This entire conversation forces a hard question. Why were we told depression was simply a chemical imbalance?
That narrative sold billions of prescriptions. It also simplified a profoundly complex human experience.
When a problem is multifactorial, a single pill is rarely the whole answer.
The tragedy is not that antidepressants exist. It’s that many patients were never given the full picture.

This isn’t an anti-medicine rant. Some patients do benefit from SSRIs.
But the data shows:
High discontinuation.
High side-effect burden.
High withdrawal rates.
Serious risks often under-discussed.
Informed consent should include all of that.

If you’re considering starting or stopping medication, A Midwestern Doctor’s article is required reading.
The report compiles trial data, metabolic models, taper protocols, and patient testimony in one place.
It challenges the dominant story.
Read it yourself and decide.
What Everyone Needs to Know About Antidepressants
Mental health deserves nuance.
Some people credit SSRIs with saving their lives. Others believe they nearly lost theirs because of them.
Both realities can exist.
The real failure is pretending the risks are negligible, the withdrawals rare, and the alternatives irrelevant.
If we want honest medicine, we need honest conversations.

The bigger question here is whether society has mistaken symptom suppression for healing.
When prescriptions rise and disability rates rise alongside them, that deserves our scrutiny. It’s okay to ask these questions.
Complex neurological problems rarely yield to simple chemical narratives.

Thanks for reading! This information was based on a report originally published by A Midwestern Doctor. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
What Everyone Needs to Know About Antidepressants
For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by A Midwestern Doctor:
The Great Alzheimer’s Scam and The Proven Cures They’ve Buried for Billions
What They Don’t Tell You About C-Sections
What’s The Healthiest Water To Drink?
While you’re at it, give A Midwestern Doctor a follow. No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed. This is easily one of the most valuable accounts you’ll ever follow.

If you haven’t subscribed to this Substack yet, take a moment to read what some of the most powerful voices in the medical freedom/truth movement have to say:
“The Vigilant Fox has been putting in a lot of work to create a news platform that shares the stories we want to hear about and brings attention to the most important things to know about.”
– A Midwestern Doctor, The Forgotten Side of Medicine
“The Vigilant Fox absolutely is on top of things. We must support our fighters, and the Fox is fighting with truth.”
– Tom Renz, Tom Renz’s Newsletter
“Excellent capture of key video presentations on evolving pandemic science.”
– Peter A. McCullough, MD, MPH, FOCAL POINTS (Courageous Discourse)

Therapists also never hear or report on those who improved, because they stop going to therapy. That said, SSRIs almost ruined our marriage, until we found the only medicine that could help - light.
Thank you so much for the very important work you do in getting this the exposure it desperately needs.