
CDC Makes Big Changes to Childhood Vaccine Schedule
This marks the largest rollback of routine childhood vaccination in U.S. history.

This article originally appeared on Focal Points and was republished with permission.
Guest post by Nicolas Hulscher, MPH
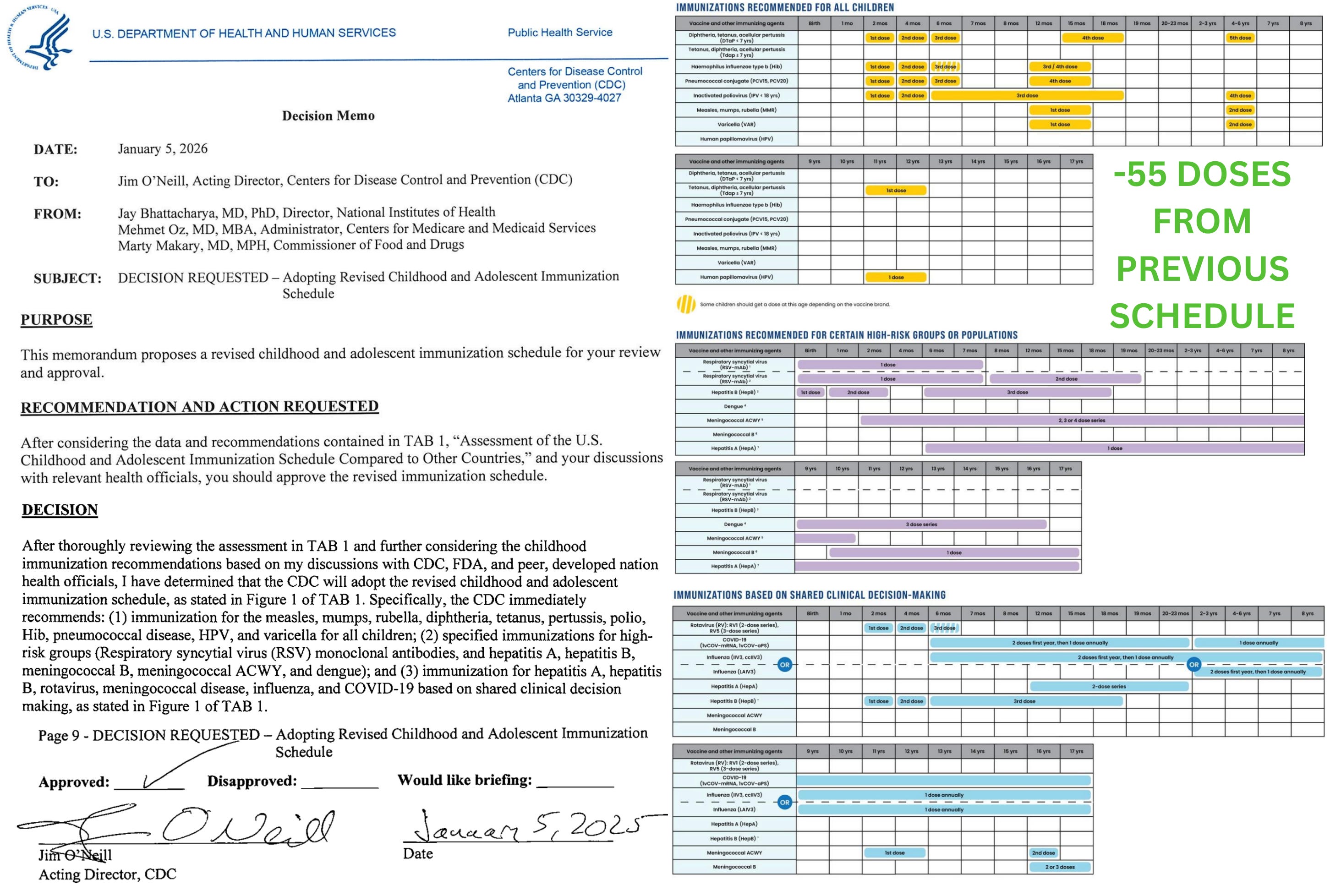
Today, the CDC formally adopted a revised childhood and adolescent immunization schedule, following a Presidential Memorandum directing alignment with international best practices.
This marks the largest rollback of routine childhood vaccination in U.S. history.
After reviewing peer-country schedules and the scientific evidence underlying them, federal health leadership acknowledged that we are hyper-vaccinating our children.
The result is a dramatically smaller routine childhood vaccine schedule, cutting approximately 55 routine doses.

This is a major victory — even as serious safety concerns remain for the vaccines that continue to be recommended.
The Key Change: ~55 Routine Doses Eliminated
Previous U.S. routine schedule (2024)
84–88 routine vaccine doses
Targeting 17 diseases
(18 if RSV monoclonal antibody is included)
New CDC routine schedule (2026)
~30 routine doses
Targeting 10–11 diseases
Based on international consensus
Net change: approximately 54–58 routine doses removed, commonly summarized as ~55 routine doses.
Importantly, this reduction applies only to vaccines previously labeled “routine for all children.” No vaccines were banned or removed from availability.
What Was Removed from the Routine Schedule
The following vaccines are no longer recommended for all children by default:
COVID-19
Influenza
Hepatitis A
Hepatitis B (including removal of the universal birth dose if the mother is HBsAg-negative)
Rotavirus
Meningococcal ACWY
Meningococcal B
These vaccines account for nearly the entire ~55-dose reduction.
What Remains Routine
The CDC now limits routine childhood vaccination to the following vaccines:
Measles, Mumps, Rubella (MMR)
Diphtheria
Tetanus
Pertussis
Polio
Haemophilus influenzae type B (Hib)
Pneumococcal disease
Varicella (chickenpox)
Human Papillomavirus (HPV), reduced from two doses to one
This is still not “safe by default”
These vaccines remain:
Insufficiently studied for long-term outcomes
Untested in placebo-controlled trials
Never evaluated as a cumulative schedule
Inducers of over 20 chronic diseases
Adverse events such as febrile seizures, severe neurological injury including autism, ADHD, tics, autoimmune disease, asthma, allergies, skin and gut disorders, ear infections, and a long list of other chronic diseases have been documented across multiple vaccines on this list:

Reducing the schedule does not equal proving safety. It simply reduces exposure. Nonetheless, that reduction alone is quite meaningful.
Where Those Vaccines Went
Non-consensus vaccines were reclassified, not banned:
Shared Clinical Decision-Making
COVID-19
Influenza
Hepatitis A
Hepatitis B
Rotavirus
Meningococcal ACWY
Meningococcal B
High-Risk Groups Only
RSV monoclonal antibody
Hepatitis A (travel, outbreaks, liver disease)
Hepatitis B (HBsAg-positive or unknown maternal status)
Dengue
Meningococcal vaccines for defined risk groups
All remain available and fully covered by insurance. However, given entrenched institutional habits and ideological adherence to maximal vaccination, many clinicians are likely to continue promoting shared clinical decision-making vaccines as de facto routine unless families are informed and assertive.
Why This Is Still a Massive Win
For decades, the childhood vaccine schedule expanded without:
Schedule-level safety trials
Long-term outcome data
Meaningful public debate
Informed consent
This decision reverses that trajectory. It:
Shrinks routine exposure dramatically
Restores parental agency
Forces future decisions to confront risk-benefit reality
Most importantly, it breaks the false premise that “more vaccines is always better.”
Conclusion
The CDC has eliminated every non-consensus vaccine from the routine childhood schedule, cutting routine exposure by approximately 55 doses—an implicit admission that the safety of the expanded schedule was never adequately established.
This decision does not end the problem. The vaccines that remain routinely recommended are still largely untested in long-term, placebo-controlled trials, are administered during critical periods of neurodevelopment, and continue to pose serious safety concerns. As a result, a substantial number of autism cases and other chronic conditions will continue to occur.
However, by sharply reducing cumulative exposure during early childhood, this change marks the first credible step toward reversing the trajectory. The burden of neurodevelopmental injury should begin to decline—not disappear, but diminish.
Even with its limitations, this action represents the most consequential course correction in U.S. pediatric vaccination policy in modern history. It breaks the assumption that an ever-expanding schedule is inherently safe, restores proportionality, and opens the door to long-overdue accountability, transparency, and real safety science.
Epidemiologist and Foundation Administrator, McCullough Foundation
www.mcculloughfnd.org
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
Copyright 2026 Focal Points

Would like to see MMR contents investigated and elucidated for both composition and uniformity. Would like to see ethical versions of MMR and Chickenpox jabs. Religious exemption is fairly straightforward for those two, by the way, and no employer, school nor government should have a word to say about imposing jabs for genital warts.
I did not have this on my bingo card.
2026 is gonna be lit!