
They Censored This in 2020: RFK Jr. on Who Gets Rich When Vaccines Go Wrong
“This is a really great business plan...”


The following information is based on a report originally published by A Midwestern Doctor. Key details have been streamlined and editorialized for clarity and impact. Read the original report here.
RFK Jr. once said: “They’re making $60 billion a year selling us vaccines, but they’re making $500 billion a year selling the remedies for the injuries caused by vaccines.”
“This is a really great business plan for [pharmaceutical] companies. You make people sick, and then you sell them the lifetime cure.”
This interview, which originally aired on September 17, 2020, was removed by YouTube for “medical misinformation.”
But was it really “misinformation,” or was RFK Jr. leading viewers to an inconvenient truth?
In just about every industry, a great product makes you rich beyond belief, except one: medicine.
The rules for enrichment work differently here. And the reason why is exactly what they don’t want you to know.
There’s a principle that I’m sure you’re familiar with: once you see it, you can’t unsee.
No industry built to solve a problem ever actually solves it. Think about it—a cure for the problem is a death sentence for the paycheck. The cancer charity that beats cancer has to close its doors. The dating app that finds you a partner just lost a paying user.
So problems don’t get solved. They get managed. Indefinitely.
And nowhere has this been turned into more of an art form than medicine.
We’re taught to see healthcare as a race toward cures. Brilliant minds, billions in research, all pointed at making disease disappear.
But that’s not how it works.
Let’s take a look at how the business model actually works. It’s actually pretty simple.
A cured patient stops paying. A managed patient pays forever.
When those two incentives collide, take a guess at which one usually wins.

Every large business chases the same things: constant growth, high markups, a captive market, and sales that repeat far into the future.
A medication you take once and never need again breaks every one of those rules.
A medication you take every day for the rest of your life satisfies all of them at once.
That’s not a conspiracy. It’s just what the math rewards.

This information comes from the work of medical researcher A Midwestern Doctor. For all the sources and details, read the full report below.
Why Medicine Won’t Cure You (and What’s Finally Changing)

If this sounds cynical, consider that Wall Street put it in writing.
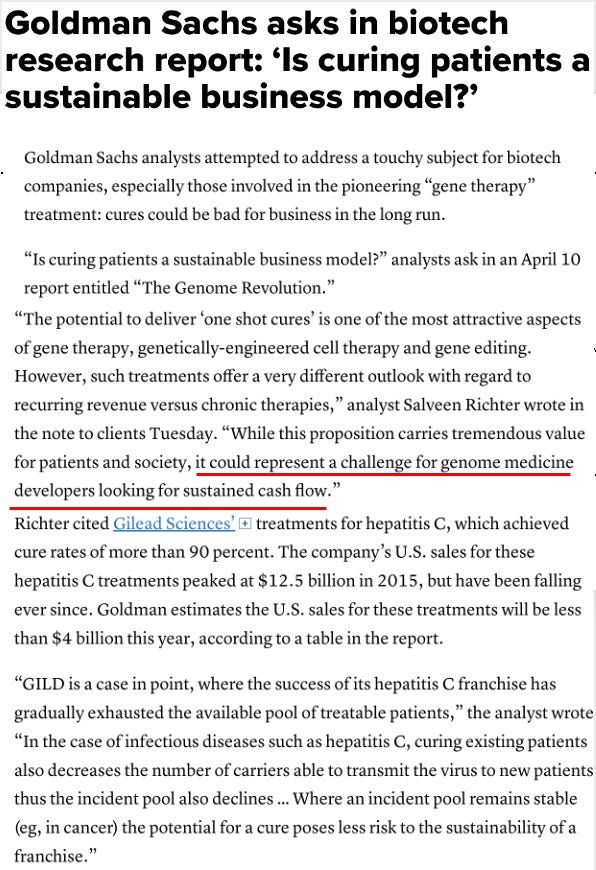
In 2018, Goldman Sachs analysts released a report on gene therapy with an almost unbelievable title: “Is curing patients a sustainable business model?”
Excuse me?!
Their concern wasn’t whether the cures worked. It was that they worked too well.
They pointed to Gilead’s hepatitis C treatment, which cured over 90% of patients. US sales peaked at $12.5 billion in 2015—then fell every year after, because the company kept running out of sick people to treat.
A cure, in other words, was a revenue problem.
Think about that.
A treatment that cured people was flagged as a business risk—because it shrank the pool of paying customers.
That’s not an accusation from a critic.
That’s the analysis a bank literally handed its investors.

The full piece traces this single idea—curing is bad for business—from Wall Street memos all the way into the language doctors are trained to use.
There’s a reason the word “cure” has quietly vanished from medicine. A Midwestern Doctor lays it out.
Why Medicine Won’t Cure You (and What’s Finally Changing)
Here’s where things get really weird…
The word “cure” has quietly disappeared from the profession. For centuries, major medical dictionaries either skipped defining it or defined it in the vaguest possible terms. It’s missing from the indexes of core references like Harrison’s and the Merck Manual.
Doctors are actively discouraged from promising a cure, especially for chronic conditions.
Some of that is reasonable—it protects patients from false hope and doctors from liability.
But it has another effect. If the profession rarely claims cures are possible, no one can be blamed for failing to deliver one.
“Managing” has become the ceiling instead of the floor.

To be clear, this isn’t an anti-medicine argument.
Some drugs are worth taking in some situations. Some conditions genuinely require lifelong treatment. Both things can be true.
The problem isn’t that medicine exists, it’s what the incentives quietly select for.

There’s a reason so many drugs need to be taken forever, and it’s built into biology.
The body is wired to maintain balance. When a drug pushes in one direction, the body pushes back the other way.
So the response to most medications tends to follow one of three paths. The effect fades unless you keep taking it. Or you need higher and higher doses for the same result. Or your body resets to a new baseline and can no longer function without the drug at all.
We can call that last one dependency.
Which is how you end up with a spectrum where nearly every successful drug sits somewhere between “addictive” and “ineffective.”

Unfortunately, drug side effects aren’t always a flaw in the system. Sometimes they’re the next product.
A drug causes a problem. That problem needs another drug. That drug causes its own problem. And so on.
In marketing, this is called a sales funnel—a cheap entry point that converts a fraction of people into something more expensive at every stage.
Once you see medicine this way, the funnels are everywhere. Literally.

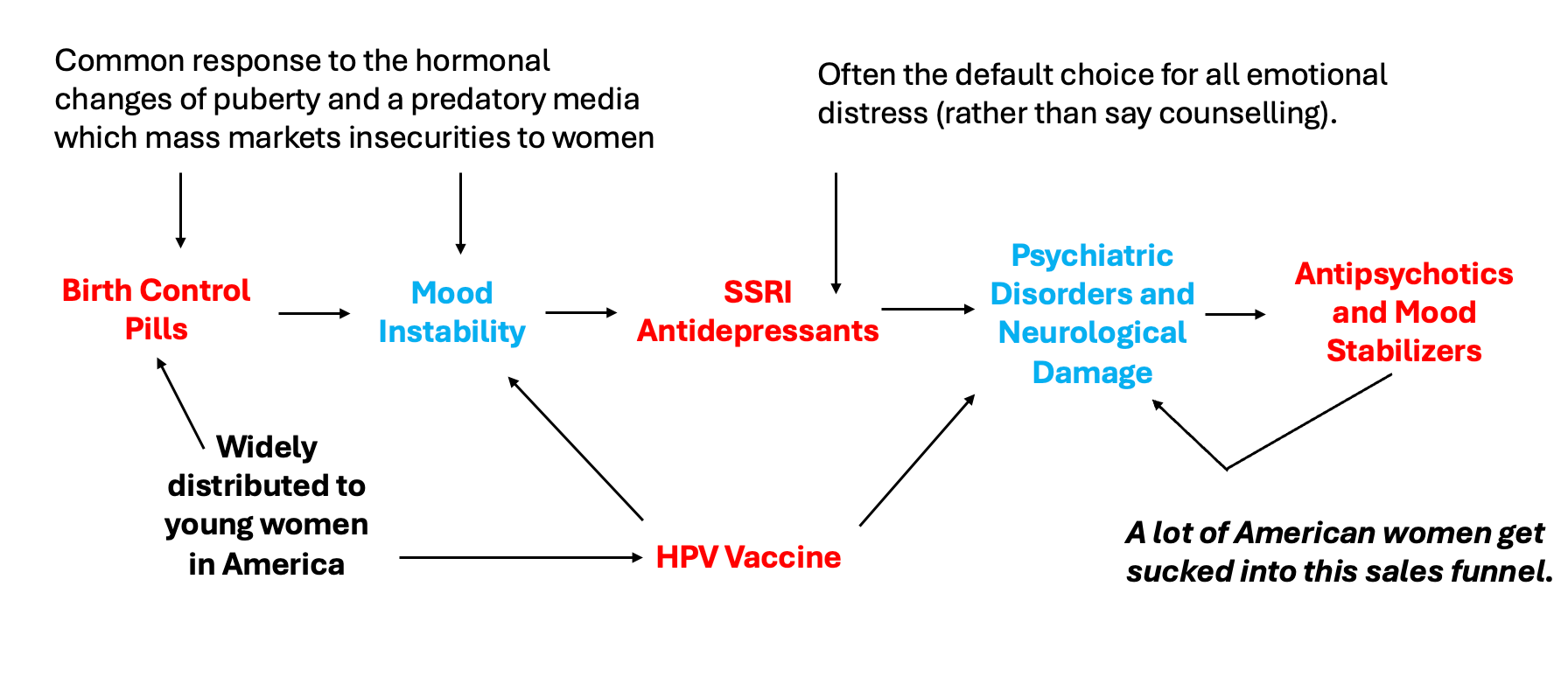
The clearest example targets American women. And it starts young.
Birth control pills, handed out widely to teenage girls, can drive mood instability. Mood instability gets met not with counseling or questions about their birth control pills, but with an SSRI—often the default response to any emotional distress.
The SSRI brings its own neurological and psychiatric fallout. And that, in turn, opens the door to antipsychotics and mood stabilizers.
Each step looks like a reasonable medical decision. Stacked together, they form a funnel a person can spend decades inside, getting more medicated at every stage.
And these aren’t niche drugs.
One in six American adults takes a psychiatric medication. Half of all adults are on at least one lifelong prescription of some kind.
That’s not a hidden corner of healthcare. That’s actually the center of it.
When a drug class reaches that scale, the incentive to keep it unquestioned becomes enormous—and so does the effort spent keeping criticism quiet.

For years, SSRIs sat in the same protected category as other drugs that quietly harmed people but made too much money to touch.
A Midwestern Doctor’s full article walks through exactly how that silence was finally broken—and the unlikely path that did it.
Why Medicine Won’t Cure You (and What’s Finally Changing)
SSRIs earn the focus for a specific reason.
They help a real subset of patients—that part is true. But at the same time they’re massively overprescribed, they frequently devastate people’s lives, and they can be extraordinarily hard to stop taking.
For decades, that last part stayed invisible. If you weren’t personally trapped on them, you’d never know how brutal getting off could be.

So how do you make an invisible problem visible?
Not with the common side effects—those are easy to ignore from the outside.
You start with the one consequence that’s too dramatic to look away from.

For years, the strongest evidence linking SSRIs to psychotic violence and mass shootings sat buried—locked inside dense academic books or scattered across sensational news clips that no neutral reader would ever trust.
The reframing was simple. The country was already at war over mass shootings and gun control. If a significant share of those shootings traced back to a drug rather than to gun laws, that was a conversation people across the spectrum had reason to engage with.
The argument finally broke through. A national segment eventually ran on the idea that prescriptions—not just firearms—might be making the situation worse.
Once that door opened, attention finally turned to the far more common, quieter harms SSRIs cause.
That shift built until it reached a place no one expected: a federal panel where SSRI victims told their stories directly.
One account went viral—a woman describing how the drugs stripped away her ability to feel love or connect physically with her partner. Not a rare side effect buried in fine print. A life quietly hollowed out.
In that moment the abstraction became real.
Then the federal government announced a multiagency effort aimed at getting people off a major drug class—not on one.
The plan: train providers to recognize inappropriate prescribing, teach them how to safely taper patients off antidepressants, reimburse them for doing it, and offer non-pharmaceutical alternatives instead.
Every previous federal health push you can name moved in the opposite direction—more prescriptions, more coverage, more uptake. This one inverts the entire logic of the system it operates inside.
To grasp how large that is: in an era when industry had less grip on the FDA, it still took more than a decade of activism, leaks, and hearings just to win a warning label noting SSRIs could cause suicide.

The pushback was immediate and revealing.
A sitting US senator responded with fury—not to a dangerous policy, but to the idea of reducing dependence on these drugs at all, insisting the government keep its hands off her medicine cabinet.
That reaction is the whole pattern in miniature.
When the proposal is fewer drugs and more recovery, the system treats it as the threat.

Take a step back and the deeper issue comes into view.
Most chronic disease follows a chain. Something harmful is present in the body. It keeps injuring. The damage accumulates. Eventually the person notices symptoms and seeks help.
The earlier in that chain you intervene, the closer you get to an actual cure.
But most pharmaceuticals act at the very last stage—muting the symptom while the underlying process grinds on. Partly by design, and partly because symptoms are simply the easiest thing to measure in a study.
So you reduce the discomfort, change nothing upstream, and take the drug forever. Which, conveniently, is exactly what the business model needs you to do.

Here’s the part that complicates the easy villain story.
This isn’t only about greed. It’s also about comfort.
Most institutions start as scrappy underdogs forced to innovate. Once they succeed, the mission often shifts from solving the problem to protecting the institution. The culture starts selecting for people who master a comfortable routine over those who disrupt it.
Greed explains a lot. Plain human complacency may explain even more.

And this isn’t unique to medicine.
Nonprofits that fundraise endlessly but never end the problem. Government programs that outlive their purpose. Contractors paid up front who deliver nothing.
The pattern repeats anywhere solving the problem would dissolve the paycheck.

The full article gets specific—including details on the natural, low-cost therapy that A Midwestern Doctor has spent years documenting, the one the FDA stonewalled for decades despite proof it worked.
It’s nearly free, treats conditions labeled “incurable,” and reportedly helped reverse a case of ALS. It’s worth reading.
Why Medicine Won’t Cure You (and What’s Finally Changing)
For all of that, something real is shifting.
The most striking thing about the SSRI effort isn’t the policy itself. It’s that it offers doctors a supported, guided way to break from the standard playbook—and to rediscover why they went into medicine at all.
Not pure reform. Not pure disruption. A third path: give people permission to practice differently, then let the results speak.

Which leads to the thought underneath all of this.
A system designed to manage problems forever will always resist solving them. Not because the people inside are evil, but because the structure rewards permanence over resolution—and most of us would rather repeat a comfortable routine than face the uncertainty real solutions demand.
That’s the trap. It isn’t only that someone profits from your staying sick. It’s that an entire system has slowly, almost unconsciously, organized itself around your never fully getting better.
The first real test of whether that can change is happening right now, with a single drug class.
What’s worth watching is whether it stays one exception—or becomes the moment the whole logic finally cracked.

Thanks for reading! This information was based on a report originally published by A Midwestern Doctor. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
Why Medicine Won’t Cure You (and What’s Finally Changing)
For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by A Midwestern Doctor:
The FDA’s 50-Year War on the Safest Painkiller Ever Discovered
What They Don’t Tell You About C-Sections
What’s The Healthiest Water To Drink?

While you’re at it, give A Midwestern Doctor a follow. No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed. This is easily one of the most valuable accounts you’ll ever follow.
If you haven’t subscribed to this Substack yet, take a moment to read what some of the most powerful voices in the medical freedom/truth movement have to say:
“The Vigilant Fox has been putting in a lot of work to create a news platform that shares the stories we want to hear about and brings attention to the most important things to know about. If you want a daily newsfeed in alignment with our ...”
– A Midwestern Doctor, The Forgotten Side of Medicine
“The Vigilant Fox absolutely is on top of things. We must support our fighters, and the Fox is fighting with truth.”
– Tom Renz, Tom Renz’s Newsletter
“Excellent capture of key video presentations on evolving pandemic science.”
– Peter A. McCullough, MD, MPH, FOCAL POINTS (Courageous Discourse)

Forbidden Facts by Gavin de Becker stated that $62.3 Billion was paid in penalties by the Medical Industry for fraud and defective products between 1990 and 2021...and it still thrived. How many billions from charities have gone into deep pockets looking for cures, which never were found? Information about Hippocrates, the Father of medicine 2400 years ago who was KNOWN for his CURES is NOT TAUGHT in med school. Hippocrates prescribed natural food, exercise, sunlight, fresh air, a change of venue, if necessary and a healthy lifestyle. He said,"Let Food be Your medicine; and Medicine be Your Food." Nutrients from food NOURISHES the glands, organs and cells providing good health. TOXIC elements in drugs and vaccines destroys the glands, organs and cells CAUSING bad health. SIMPLE TRUTH won't put enough money into anyone's pockets..
There is no profit in health.