
The Troubling Reality of How Millions End Up on Blood Pressure Drugs
It sounds unbelievable, but it is very real.


The following information is based on a report originally published by A Midwestern Doctor. Key details have been streamlined and editorialized for clarity and impact. Read the original report here.
Nurses have a common saying in medicine:
When patients go unresponsive, or their vital signs become dangerous, it often happens 30 minutes AFTER they take their blood pressure pills.
For decades, doctors have mindlessly put tens of millions on BP meds without ever considering why their blood pressure is high to begin with.
In 90–95% of cases, people are diagnosed with high blood pressure and put on medication with “no known cause.”
Blood pressure is treated as the problem itself, not a signal of an underlying issue.
And that’s where everything starts to go wrong.
Blood pressure is treated like one of the clearest, most settled things in medicine.
If the number is high, lower it.
If the number drops—success!
But there’s a growing argument that blood pressure may often be a signal that something deeper is wrong with circulation, not the root problem itself.
And when medicine fixates on the number instead of the cause, people can get labeled, medicated, and harmed in the process. All while the root cause is completely missed.
The first crack in that story is surprisingly simple.
90–95% of hypertension cases are classified as “essential hypertension.”
That’s a technical way of saying: elevated blood pressure without a known cause.
Wait just a minute.. we’ve built an entire treatment system around a condition that, in most cases, medicine still cannot actually explain?
That alone should raise eyebrows.

This information comes from the work of medical researcher A Midwestern Doctor. For all the sources and details, read the full report below.
Understanding Blood Pressure in a Healthy Way

And yet the diagnoses—and prescriptions—just keep growing.
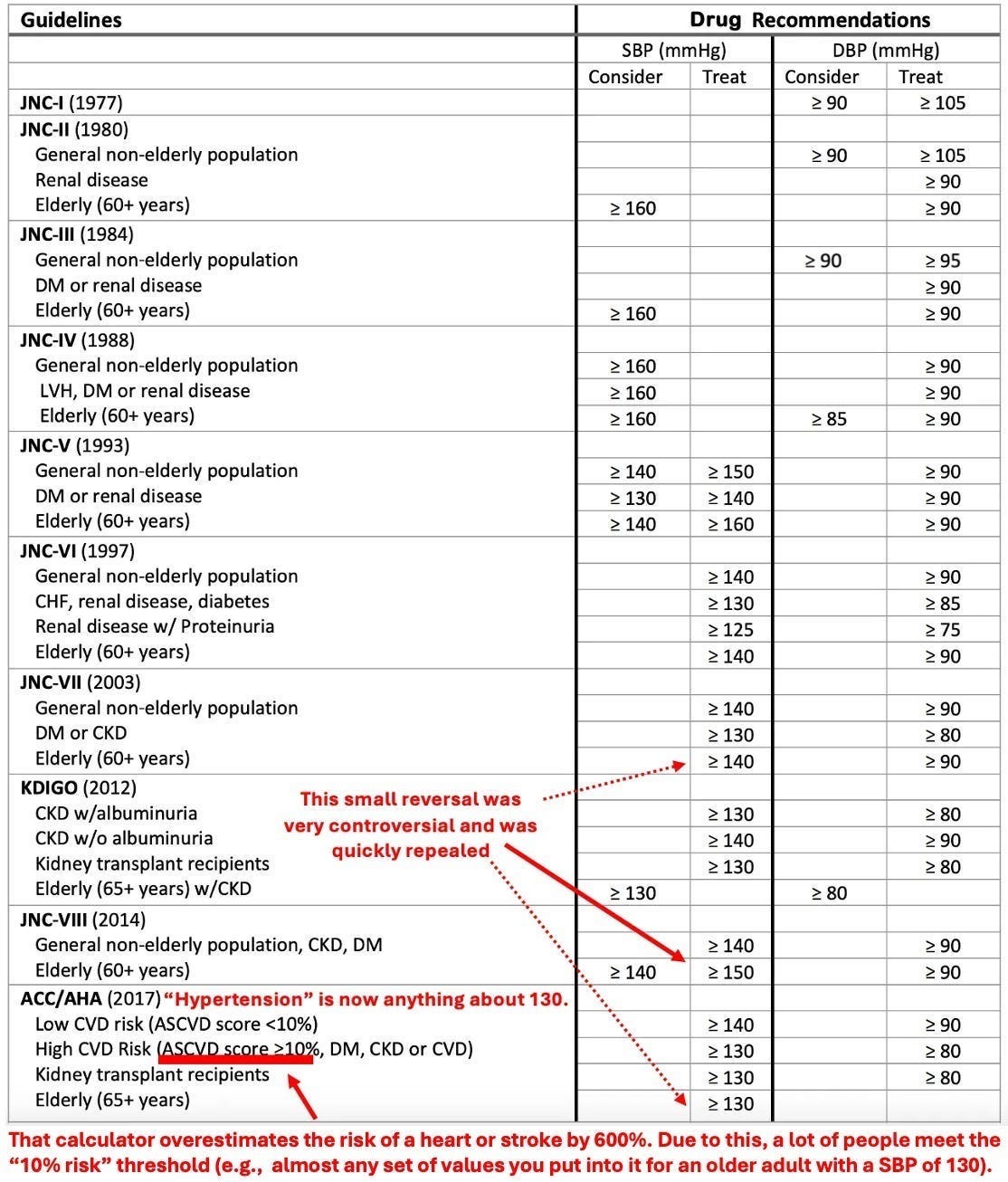
When blood pressure thresholds are lowered, more people suddenly qualify as hypertensive.
It’s amazing how that happens.
One guideline shift alone moved the U.S. from 32% to 46% of adults being labeled with high blood pressure.
That’s not a gradual trend.
That’s millions of people becoming “patients” in a matter of seconds simply because the definition changed.
It sounds unbelievable, but it is very real.
Here’s where it gets even more uncomfortable.
Blood pressure is highly variable, especially where it’s typically measured—in the arm.
I’m sure you’ve had the cuff put on more than a few times. Do you ever feel nervous or a little uncomfortable when it’s happening?
Something called “white coat hypertension” affects 15–30% of diagnosed patients.
That means the stress of being in a doctor’s office and of having your blood pressure measured can temporarily spike readings high enough to trigger a diagnosis.
And once that label sticks, it rarely goes away.
Uh oh.

But it doesn’t stop there.
Measurement errors are common—wrong cuff size, differences between arms, improper cuff or body positioning.
Estimates suggest around 25% of hypertension diagnoses are incorrect.
25%.
Think about that.
A significant number of people may be put on lifelong medication based on readings that were never reliable to begin with.
That’s horrible.

What if “high blood pressure” is less of a disease and more a warning signal?
A Midwestern Doctor’s report breaks down why the number alone may not tell the full story—and what might actually be driving it.
Understanding Blood Pressure in a Healthy Way
The deeper issue comes down to circulation.
Blood pressure isn’t just a random number—it reflects how blood moves through the body, which is a very important indicator of health.
When arteries stiffen or blood flow is impaired, the body may raise pressure to compensate.
In that sense, higher pressure might not always be the problem.
It might be the body trying to solve the problem.

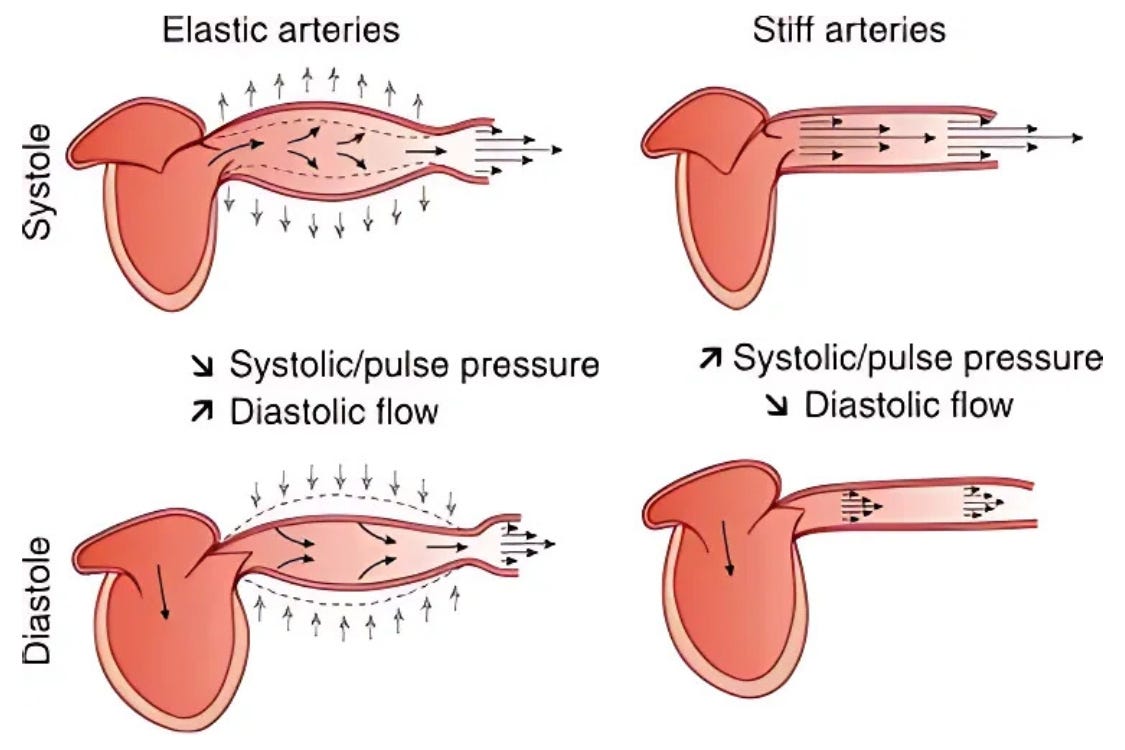
Picture two arteries.
A healthy one stretches easily, absorbs pressure, and keeps blood moving.
A damaged one can’t stretch. Pressure builds. Blood slows. The heart has to push harder.
Now ask yourself: Is the pressure the cause of the problem, or is it the result of a system under strain?
At a basic level, blood pressure comes down to two things:
How much blood is in the arteries, and how tight or relaxed those arteries are.
That’s it.
And most medications work by manipulating those two levels—loosening vessels, reducing blood volume, or weakening the heart’s contraction.
Same number.
Very different biological effects.

This matters more than people realize.
Because lowering a number doesn’t automatically fix the underlying issue.
You can absolutely reduce pressure without improving circulation.
So you hit the target (yay!) without restoring function (boo!).
Those are not the same thing. And pretending they are can be a big mistake.

Another overlooked factor: where the pressure is measured.
The number most people know comes from the arm. We’ve all experienced the cuff. Maybe you even have one at home.
But central blood pressure, inside the aorta, is more closely tied to cardiovascular outcomes.
And the readings from the those two locations can differ significantly.
So the number guiding most treatment decisions may not even reflect the pressure that matters most!

A blood pressure reading may seem precise, but it can fluctuate, mislead, and even misdiagnose.
Once thresholds drop, a borderline reading can suddenly turn into a lifelong condition.
This is a topic everyone needs to understand and be prepared for. You never know when your routine reading will suddenly be “too high.”
Understanding Blood Pressure in a Healthy Way
Over time, treatment guidelines have steadily lowered the definition of “high.”
Each shift pulls more people into the treatment pool.
But at some point, we need to ask the question, are we detecting more disease or redefining what counts as normal?
The effect becomes especially obvious with age.
A large majority of people over 75 now meet the criteria for hypertension.
And most meet the threshold for medication. Which is great for Big Pharma, by the way.
When nearly everyone in a group is labeled abnormal, it forces a rethink of the model itself.
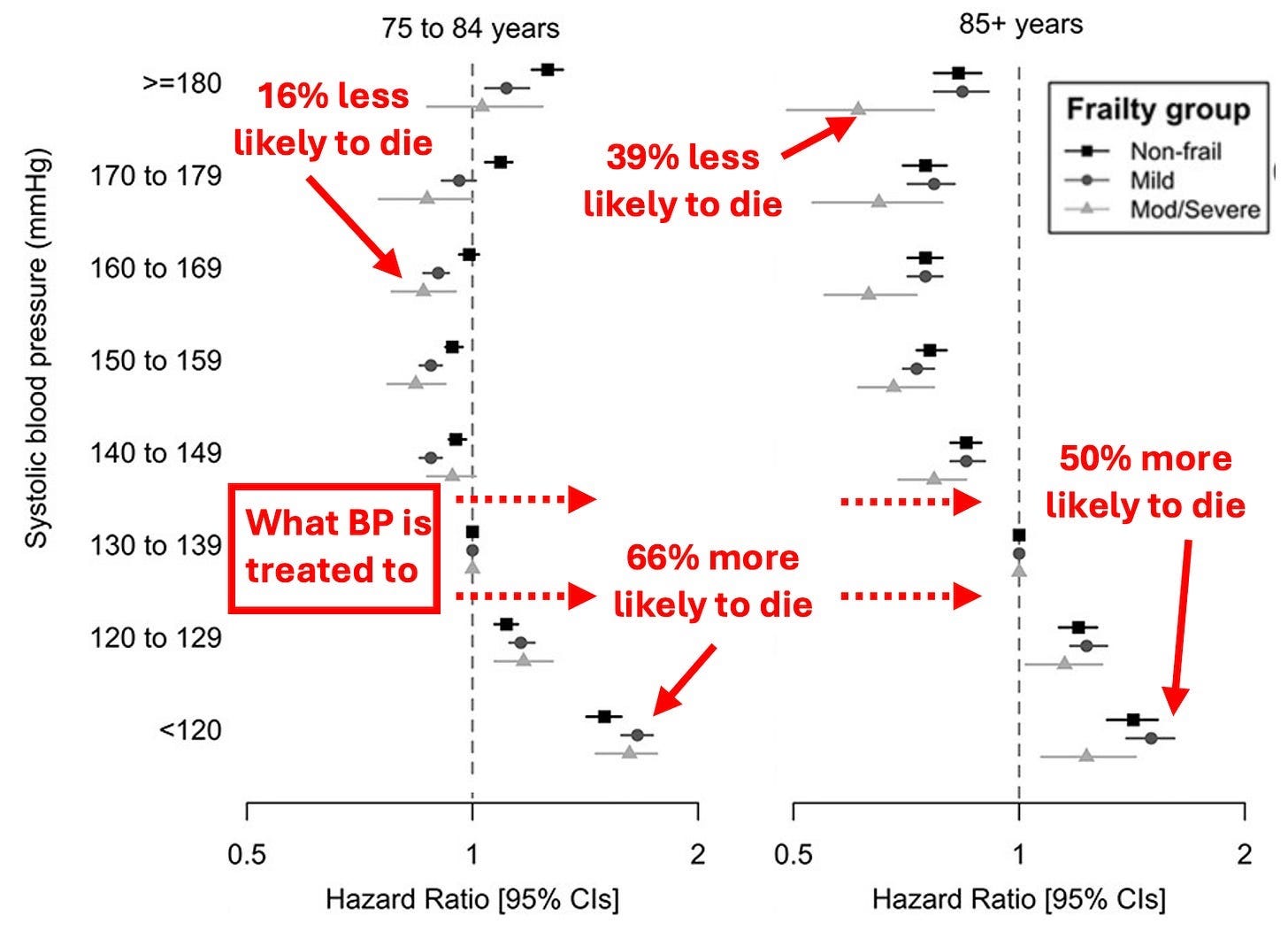
That might be manageable if treatment carried little risk. But interventions don’t usually come without risk.
Lowering blood pressure too aggressively can reduce blood flow to vital organs.
The brain.
The kidneys.
The heart itself.
And those systems depend on steady perfusion to function.

In older adults, that tradeoff becomes clearer.
In one large study of people over 70 with hypertension, 9% experienced serious falls and 16.9% died over a three-year period.
Lowering pressure isn’t always neutral.
In some cases, it can destabilize the very systems it’s meant to protect.

There’s also kidney risk.
Some blood pressure drugs increase the likelihood of acute renal injury.
And in patients with advanced kidney disease, lower blood pressure has been linked to higher mortality.
That flips the usual assumption on its head.
Lower isn’t always safer.

Plus, not all blood pressure drugs are equal.
Different classes can produce very different outcomes—even when they lower blood pressure by the same amount.
Some reduce cardiovascular events. Others don’t.
Which suggests something important: the benefit may not come from lowering the number itself.
If two drugs produce the same drop in blood pressure but lead to very different health outcomes, then blood pressure alone can’t be the full story.

The side effects are also far from uniform.
Some drugs dehydrate the body and disrupt electrolytes.
Others slow the heart and affect energy levels.
Some increase swelling, dizziness, or digestive issues.
And others come with more serious risks tied to kidneys or metabolism.
These aren’t minor differences.
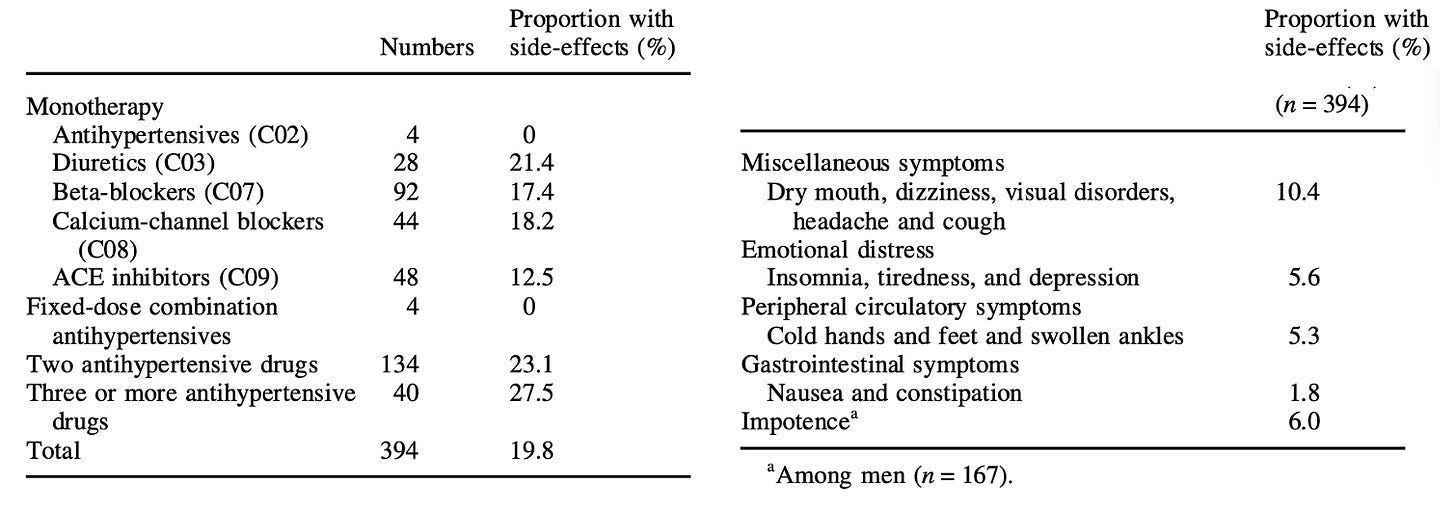
Side effects are often described as rare or manageable. But real-world behavior tells a different story.
When large numbers of patients stop taking these drugs, it raises a question: what are they experiencing that isn’t being fully acknowledged?
A Midwestern Doctor asks this question and more in the full article.
Understanding Blood Pressure in a Healthy Way
In a study of 370,000 patients under 65, 23.5% stopped taking blood pressure medication within 270 days.
Among those who continued, 40.2% often skipped doses.
That’s not a small minority. That’s a pattern.
And patterns usually point to something real.

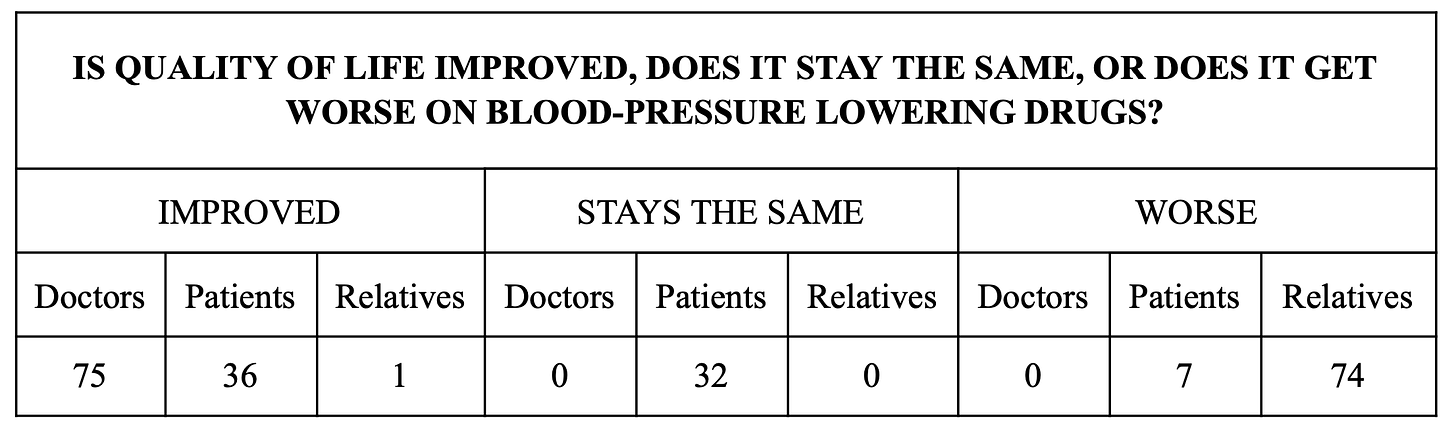
There’s also a perception gap.
When researchers compared how doctors, patients, and families viewed the effects of these medications, the differences were striking.
Doctors often saw improvement.
Patients were less convinced.
Families frequently reported things getting worse.
Same treatment. Very different lived experience.
This alone raises some important questions that we really should be asking.
A deeper issue here may be how medicine approaches the problem itself.
Blood pressure is easy to measure. But perfusion, circulation quality, and vascular health are harder.
So the system focuses on what it can quantify—even if that number doesn’t tell the full story.

And that leads to a broader tension.
If most hypertension has no clear cause, if diagnoses can be unstable, if thresholds keep expanding, and if lowering the number can sometimes create new risks… Then what exactly is being optimized?
The patient’s health? Or the measurement itself?

That question doesn’t have an easy answer, but it points to something really important.
Health isn’t always captured in a single number.
And when a system treats numbers as targets instead of signals, it risks missing what the body is actually trying to say.
And I have a feeling our bodies often have a lot to say if we just knew how to listen.

Thanks for reading! This information was based on a report originally published by A Midwestern Doctor. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
Understanding Blood Pressure in a Healthy Way
For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by A Midwestern Doctor:
The Great Cholesterol Scam and The Dangers of Statins
Where Are the Former FDA Commissioners Now?
What’s The Healthiest Water To Drink?
While you’re at it, give A Midwestern Doctor a follow. No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed. This is easily one of the most valuable accounts you’ll ever follow.

If you haven’t subscribed to this Substack yet, take a moment to read what some of the most powerful voices in the medical freedom/truth movement have to say:
“The Vigilant Fox has been putting in a lot of work to create a news platform that shares the stories we want to hear about and brings attention to the most important things to know about. If you want a daily newsfeed in alignment with our ...”
– A Midwestern Doctor, The Forgotten Side of Medicine
“The Vigilant Fox absolutely is on top of things. We must support our fighters, and the Fox is fighting with truth.”
– Tom Renz, Tom Renz’s Newsletter
“Excellent capture of key video presentations on evolving pandemic science.”
– Peter A. McCullough, MD, MPH, FOCAL POINTS (Courageous Discourse)

The best blood pressure medicine that's also free?
Sunshine - dilates blood vessels by increasing nitric oxide. Get out there!
Few years ago, at 76, new doctor, BP reading when I first went in, always a bit high because I hate being in a doctor's office. Explained that, waited a bit, new reading nice and low. During the 'interview" given by a nurse, she asked me what prescriptions I took, i said none, she said well, what do you take to have such a nice BP reading. I said I take deep breaths and imagine myself somewhere else. I know what a prescription is.
As a side note, I said I had tried gabapentin a few years back, it just made my leg muscles cramp horribly. At the end of the appointment, the doctor said hey I am going to prescribe gabapentin for you - no one knows how it works. WTF. Actually, I think it interrupts messages from nerves to brain or something like that. I told the pharmacy to put it back on the shelf and am still looking for a new doctor.