
The Real Risks of Giving (or Skipping) the Hepatitis B Shot for Your Baby
A vaccine for a blood-borne disease became routine on day one of life. Why?


The following information is based on a report originally published by A Midwestern Doctor. Key details have been streamlined and editorialized for clarity and impact. Read the original report here.
Before the hepatitis B vaccine was mandated for kids to attend school in almost all 50 states, the risk of a baby dying from hepatitis B was 1 in 7 million.
“That means you need to give 7 MILLION hepatitis B vaccines to prevent ONE death,” RFK Jr. says.
When you give 7 million vaccines to save one life, you’d better make damn sure it’s safe.
But is it really? Let’s take a look at the evidence.
Every newborn in America is pushed toward a Hepatitis B vaccine within hours of being born.
And that sounds completely normal to most people because the policy has been normalized for decades.
But when you take a close look at Hepatitis B, the risk group, the benefit math, and the forgotten safety record, the birth-dose policy becomes very difficult to defend.

Hepatitis B is a real disease.
Chronic infection can damage the liver, lead to liver failure, and increase the risk of liver cancer later in life.
That part is not the dispute.
The dispute is whether every newborn, including babies born to mothers who test negative for Hepatitis B, should receive the vaccine on their very first day of life.

This information comes from the work of medical researcher A Midwestern Doctor. For all the sources and details, read the full report below.
Why is Every Newborn Forced to Get A Hepatitis B Vaccine?

Hepatitis B isn’t spread like measles and other contagious diseases children are routinely vaccinated for.
It generally requires blood-to-blood exposure, sexual exposure, the use of contaminated needles, accidental blood exposure, or transmission from an infected mother during childbirth.
For the average newborn baby, the serious risk is overwhelmingly tied to one scenario and one scenario only: the mother has Hepatitis B and transmits it during birth.
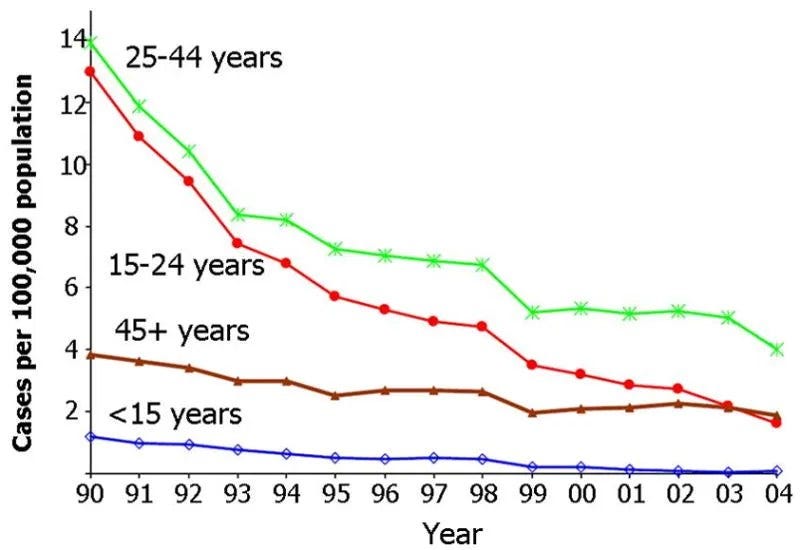
Besides that one scenario, there the risk to infants and young children is virtually nonexistent compared to every other age group.
But the official justification for the vaccine depends on a long chain of events.
The mother has to be infected.
Screening has to miss it.
The infection has to be transmissible.
Transmission has to happen during birth.
The infant infection has to become chronic.
Then, years later, it has to become consequential.
When every step is rare, the benefit shrinks—fast.
But are parents told that the stars basically must align just so for this to even be an issue for their child?

Using official-type assumptions, the math is brutal.
Roughly 0.1% of mothers have Hepatitis B.
Only a fraction have the higher-risk HBeAg-positive form.
Transmission risk varies sharply by maternal status.
And the vaccine isn’t even 100% protective.
When multiplied out, more than one million infants must be vaccinated to prevent one consequential case.
The full article asks one uncomfortable question: if the birth dose is mainly meant to prevent mother-to-child transmission, why is it still pushed on babies whose mothers test negative?
That’s where this story gets hard to explain.
Why is Every Newborn Forced to Get A Hepatitis B Vaccine?
The strongest argument for the birth dose is missed screening.
That is the idea: vaccinate everyone because a small number of maternal infections could be missed.
But that’s very different from saying every newborn faces meaningful risk.
It means a universal medical intervention is being used to cover a rare failure in screening.

This is where targeted protection becomes the obvious alternative.
If a mother is Hepatitis B positive, the infant is in a real risk category and should be handled with seriousness.
But if the mother is negative, the risk profile changes completely.
A blanket policy treats both babies almost the same.

The historical record makes the policy even more disturbing.
In 1998, Science reported growing controversy around autoimmune disease claims and France suspended school-based Hepatitis B vaccination after thousands sued the government.
In 1999, ABC News aired a major criticism of the vaccine.
That same year, Congress held hearings that almost nobody talks about today.
At that 1999 hearing, the contrast was staggering.
VAERS had reportedly received more than 8,000 adverse event reports involving the Hepatitis B vaccine, including 43 deaths in children under 2 in 1997.
By comparison, the hearing cited 95 or fewer annual Hepatitis B cases in young children and no infant deaths.
That’s the kind of risk-benefit contrast that should have triggered a serious national pause.
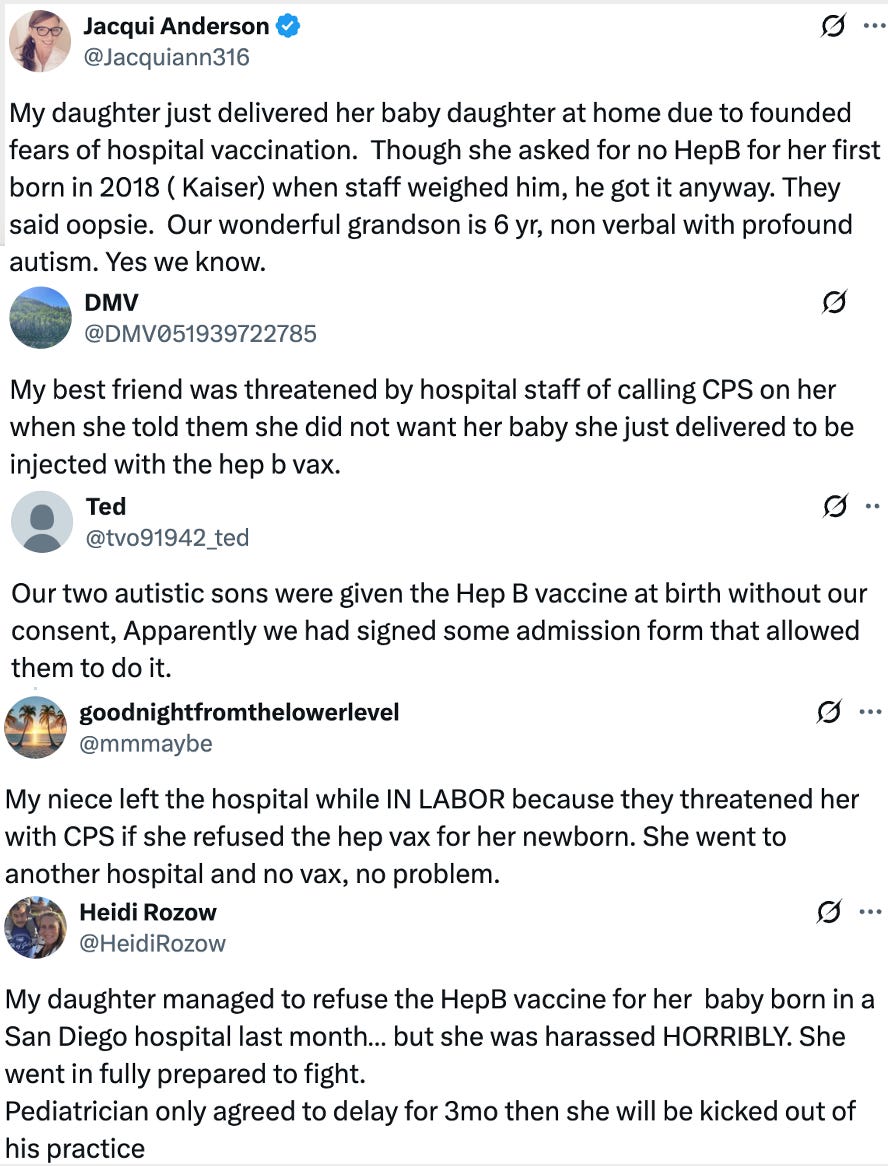
Parents also testified that the policy was being carried out without informed consent.
Some said babies were vaccinated without parental approval.
Others described coercion, pressure, and even threats involving social services.
That changes the debate.
This is no longer just about immunology. It’s about whether parents are actually being allowed to make an informed medical decision.
Then there’s the clinical trial problem.
The article argues that the original safety trials often monitored adverse events for only 4 to 5 days and did not use true inert placebos.
That window is wildly inadequate for autoimmune disease, developmental regression, demyelinating disorders, or chronic neurological problems.
You simply cannot rule out long-term harm by looking for a few days. It is literally impossible.

Even inside those short windows, the newborn adverse event numbers were not nothing.
Within 48 hours, there are reports of pain, redness, swelling, irritability, vomiting, diarrhea, feeding difficulties, drowsiness, restlessness, and fever.
In an adult, some of those may sound minor. But in a newborn, feeding problems, fever, and excessive drowsiness can become major events quickly.

A vaccine given on day one of life was cleared with short safety windows, limited follow-up, and no true placebo standard.
That alone should make people ask harder questions.
A Midwestern Doctor’s article is a must read.
Why is Every Newborn Forced to Get A Hepatitis B Vaccine?
For decades, critics raised concerns that the Hepatitis B vaccine could trigger autoimmune and demyelinating disorders.
Those concerns were dismissed as unproven.
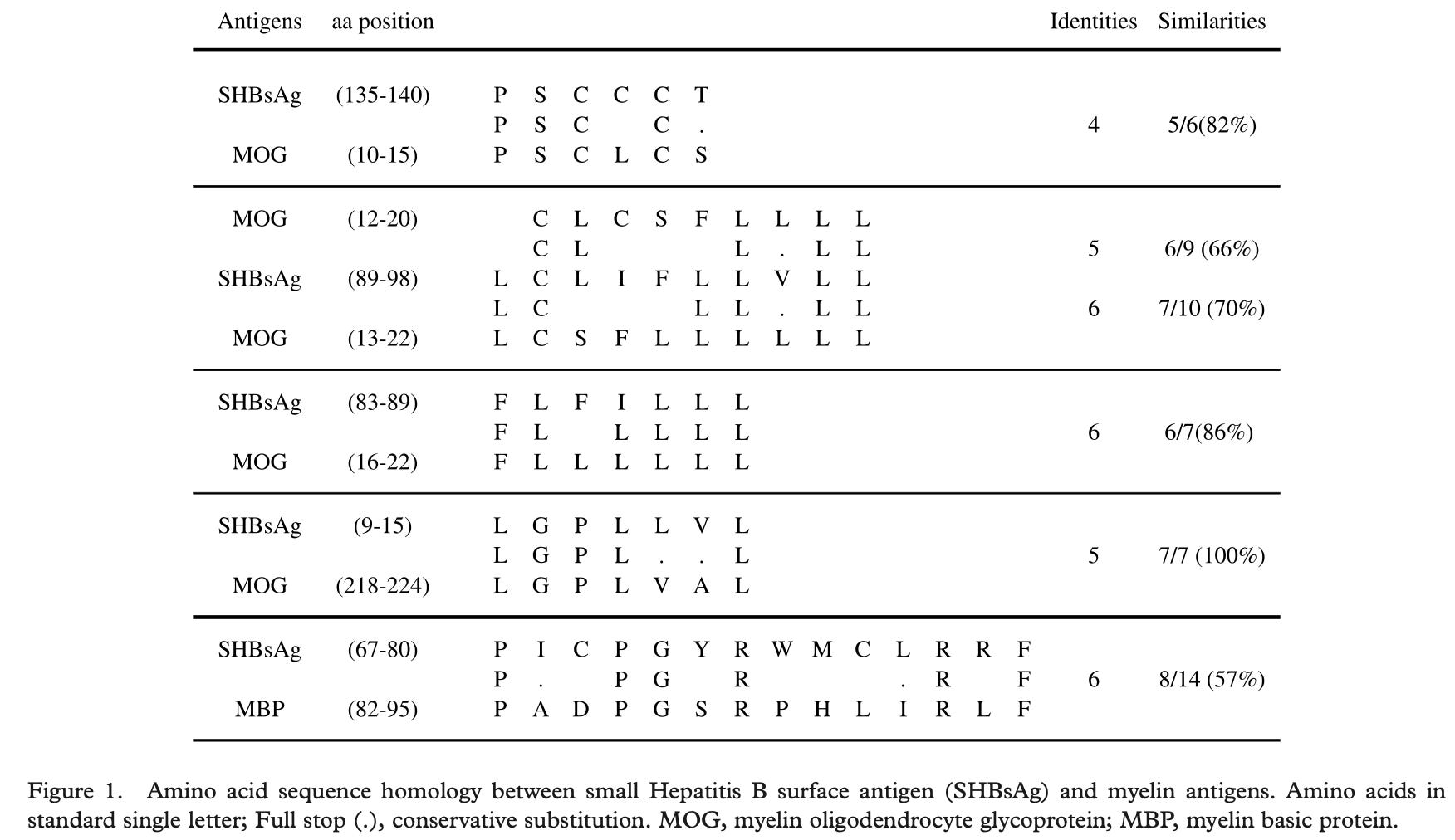
There’s one mechanism that could make that concern biologically plausible: molecular mimicry.

Molecular mimicry is simple in concept.
If an immune-provoking substance resembles human tissue, the immune system may attack both.
In this case, the concern is myelin, the protective coating around nerves.
A 2005 study found significant overlap between the Hepatitis B surface antigen and myelin, with 60% of recipients developing immune reactivity to myelin.
That should have led to major follow-up research.
Instead, the official posture remained familiar: not proven, more research needed, no reason to change policy.
That response is a clear pattern.
When patients report harm, the data are considered anecdotal.
When long-term studies are missing, the absence of proof is treated like proof of safety.

The developmental-disability data may be the most explosive part of this entire issue.
Several studies have reported associations between newborn Hepatitis B vaccination and increased risks of developmental disability, autism, or developmental delay.
Those findings are obviously controversial. But controversy is not a reason to bury the question.
When a medical intervention is given on day one of life, the burden should absolutely be on public health authorities to prove the risk is not there.

The official story says the newborn Hepatitis B shot is settled science.
The forgotten record says something else entirely.
And A Midwestern Doctor has all the details in the full article.
Why is Every Newborn Forced to Get A Hepatitis B Vaccine?
Animal studies add another layer.
In one monkey study, vaccinated infants reportedly showed delays in rooting, snout, and suck reflexes, which are some of the earliest behaviors tied to feeding and development.
A mouse study reported impaired neurogenesis, impaired behavior, disrupted hippocampal long-term potentiation, and increased brain inflammation.
No single study settles the debate.
But together, they raise questions that should have been investigated aggressively, especially before making this a day-one policy for every newborn.

The population-level data create another problem.
Acute Hepatitis B cases dropped after vaccination campaigns, and public health officials often treat that as proof of success.
But Hepatitis C fell in a similar pattern despite no Hepatitis C vaccine.
And chronic Hepatitis B prevalence sits around 0.003% with no meaningful change since 1976.
That’s a major contradiction.
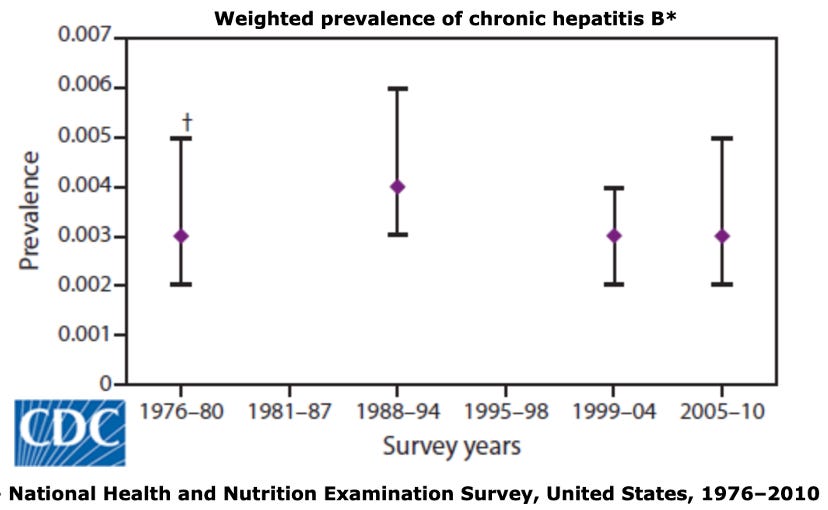
If the real target is chronic Hepatitis B, the key question isn’t whether acute infections fell.
The key question is whether the birth-dose policy meaningfully reduced chronic infection in the population.
And that target appears not to have moved.
That matters because the newborn shot isn’t being justified as a short-term case-reduction tool.
It’s being justified as lifelong protection from severe chronic disease, and the population-level data raise a much harder question about whether that promise was actually delivered.

We may never get to the bottom of why this vaccine is pushed on every newborn in America. But regardless of the reason, one thing is clear: the Hepatitis B birth dose should not be treated as a sacred ritual.
The honest position is simple: protect infants born to infected mothers with serious, targeted protocols, including screening, immune globulin when indicated, and vaccination, if appropriate.
But a blanket day-one policy for babies born to Hepatitis B negative mothers rests on much, much weaker ground.
The debate isn’t whether Hepatitis B exists.
The debate is whether a newborn’s first medical act should be a one-size-fits-all intervention with tiny benefit, disputed safety signals, and decades of unanswered questions.

Thanks for reading! This information was based on a report originally published by A Midwestern Doctor. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
Why is Every Newborn Forced to Get A Hepatitis B Vaccine?
For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by A Midwestern Doctor:
We Now Know How The Government Lied About the COVID Vaccines
The Hidden Dangers of Hospital Births & How to Protect Your Family
What’s The Healthiest Water To Drink?

While you’re at it, give A Midwestern Doctor a follow. No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed. This is easily one of the most valuable accounts you’ll ever follow.
If you haven’t subscribed to this Substack yet, take a moment to read what some of the most powerful voices in the medical freedom/truth movement have to say:
“The Vigilant Fox has been putting in a lot of work to create a news platform that shares the stories we want to hear about and brings attention to the most important things to know about. If you want a daily newsfeed in alignment with our ...”
– A Midwestern Doctor, The Forgotten Side of Medicine
“The Vigilant Fox absolutely is on top of things. We must support our fighters, and the Fox is fighting with truth.”
– Tom Renz, Tom Renz’s Newsletter
“Excellent capture of key video presentations on evolving pandemic science.”
– Peter A. McCullough, MD, MPH, FOCAL POINTS (Courageous Discourse)

There are 2 reasons why newborns receive vaccines, which they do not need and should not receive at all.
First, vaccine manufacturers have no product liability, so they cannot be sued for injuries.
Second, because of point 1 above vaccines are their profit center, 100% profit, absolutely no financial risk because they can't be sued for injury. It's disgusting.
No child needs a hepatitis b shot.
This article and the true reality nauseates me for young mothers. They have to make decisions that will likely be scrutinized and disparaged by their pediatrician.