
The Real Causes of ED and the Fixes That Actually Work
If you want to resolve your erectile dysfunction for good, Dr. Mark Hyman says you ultimately have to do this.


The following information is based on a report originally published by A Midwestern Doctor. Key details have been streamlined and editorialized for clarity and impact. Read the original report here.
66-year-old medical doctor Mark Hyman ran an experiment on himself.
He started eating more saturated fat. His testosterone levels went “way up.”
A low-fat diet, he says, does the opposite. He calls it “bad news.”
And low testosterone is never just about testosterone. It’s a “clue for other problems.”
“There’s a strong relationship between low testosterone and erectile dysfunction,” Dr. Hyman said.
Men with low testosterone are also 38% more likely to die of a cardiovascular event like a heart attack or stroke.
So doctors reach for the little blue pill. Which was never designed for ED at all. It was a failed blood pressure drug.
It doesn’t touch the root cause.
If you want to resolve your erectile dysfunction for good, Dr. Hyman says you ultimately have to fix your metabolic health.
But what if your metabolic health is fine and the problem is still there?
“Certain medications, by the way, can mess up your libido”…
Quick history lesson: for most of modern medicine, erectile dysfunction wasn’t called erectile dysfunction. It was called “impotence,” a word that manages to be a diagnosis, an insult, and a life sentence all in one.
Congratulations, you've failed at being a man, please schedule a follow-up.
Clearly nobody sat down and workshopped that word thinking about the patient’s feelings.
It set the tone for how this condition was handled for decades—and not in a good way.
Doctors rarely hear about erectile dysfunction—or ED—directly from patients. Usually it comes from a frustrated spouse, or a man mentioning, almost in passing, that some unrelated treatment “happened” to fix it.
Men just don’t bring it up.
And studies confirm what most physicians already suspect: embarrassment keeps this condition hidden, especially from female doctors.
But that silence has bigger consequences than most people realize.

This information comes from the work of medical researcher A Midwestern Doctor. For all the sources and details, read the full report below.
The Simple Ways to Restore Sexual Health

For years, ED was treated primarily as a psychological problem. That framing put the burden back on the man, right when he’d finally worked up the nerve to say something about it.
Then Pfizer changed the conversation.
But let’s be clear. It wasn’t out of concern. It was to sell Viagra.
They funded major efforts to reframe ED as a circulatory issue. Because it happened to be more profitable that way.

A Midwestern Doctor did a deep dive into the physiology of erectile dysfunction and the overlooked drug and injury causes doctors rarely explain. The full piece maps exactly how each cause disrupts the process.
The Simple Ways to Restore Sexual Health
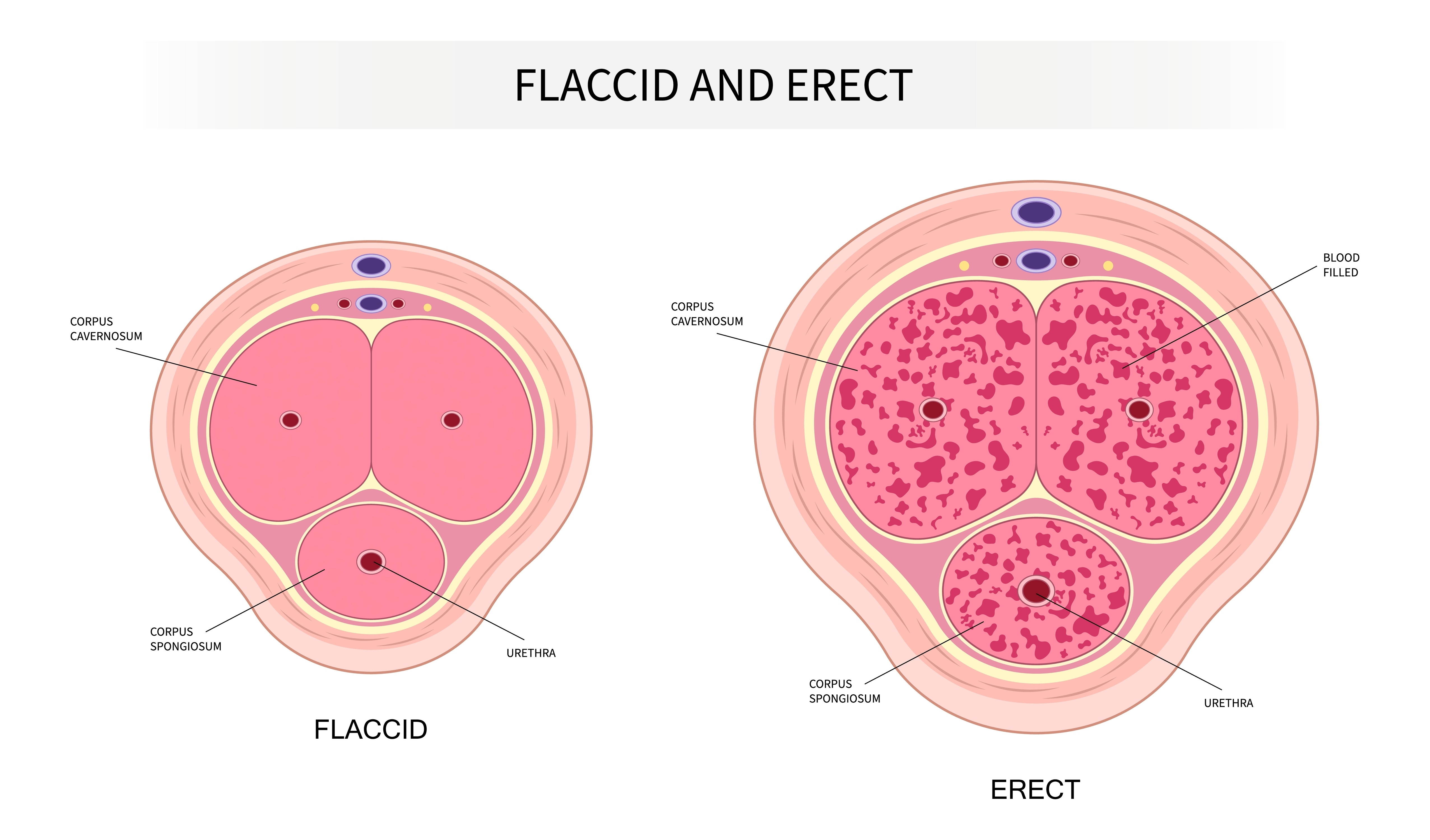
An erection is, mechanically, a hydraulic event.
Two columns of spongy tissue inside the penis fill with blood when smooth muscle around them relaxes. Nitric oxide triggers that relaxation. Blood rushes in, presses the draining veins shut, and the erection holds.
Viagra doesn’t create this signal. It just prevents the signal from breaking down once arousal is already present.
That’s an important distinction.
A pill that preserves a signal is not the same as a pill that fixes what’s disrupting the signal in the first place.

Poor circulation is the single most common cause of ED, and it usually shows up early.
In men with advanced heart disease, ED was present before the heart attack in 64% of cases.
The vessels feeding the penis are smaller than the ones feeding the heart, so they clog first.
That means ED is often not the problem. It’s the warning.
Diabetes. High blood pressure. Smoking. Obesity. Atherosclerosis.
All of it tends to show up here first.

Medications are an enormous, underappreciated cause of ED, and prescribing doctors rarely connect the two.
Beta-blockers, common blood pressure drugs, are well known for this. But the numbers on SSRIs are harder to pass over. One study of 1,022 previously healthy patients found 59% developed sexual dysfunction after starting the drug, with 31% experiencing ED specifically.
A subset never fully recovers, even after stopping.
It’s now recognized as its own condition: Post-SSRI Sexual Dysfunction.

This isn’t an argument against treating depression. Some patients need these medications.
But patients absolutely deserve to know this risk exists before they start.

There’s actually a specific protocol for using DMSO to treat ED directly.
A Midwestern Doctor breaks down the full mechanism, dosing, and combinations in the article. Subscribe to see it all.
The Simple Ways to Restore Sexual Health

Finasteride, prescribed for hair loss and prostate enlargement, works by neutralizing testosterone. And it carries a documented risk of lasting ED.
GnRH agonists like Lupron go further. Used for prostate cancer and, increasingly, for suppressing puberty, they shut down the body’s hormone production almost entirely. One study found a 267% increase in ED among men taking them. Another found 80% reported impotence outright.
These aren’t fringe side effects buried in fine print. They’re common outcomes of shutting down a hormonal system the body depends on.

But medications and circulation aren’t the whole picture.
The signal for an erection originates in the sacral nerves. Anything compressing them, spinal stenosis, disc disease, pelvic surgery, diabetic neuropathy, can produce ED even when blood flow is completely normal.
A tight, spasming pelvic floor does something similar. It physically compresses the arteries and nerves supplying the penis.
It’s common, and it’s badly underdiagnosed.

Then there’s Peyronie’s disease: fibrous scar tissue forming inside the penis, causing curvature, pain, or shortened blood flow.
It’s estimated to affect roughly 10% of men. Only 0.5 to 1% ever get formally diagnosed, because most never seek care.
In a study of 386 men undergoing ultrasound for ED, without any visible curvature or palpable plaques, 10.6% still had detectable Peyronie’s scarring. Nearly three-quarters of them had ED as their primary complaint.
Undiagnosed scar tissue, quietly reducing blood flow, in men who had no idea it was there.
That alone should change how ED gets worked up in a clinic.

Consider these stories…
A 75-year-old man with no history of ED applied a topical solution for unrelated pelvic pain. Within minutes, without any arousal, without any stimulating thought, he had a full erection. He wasn’t looking for that outcome. He was just following his usual pain routine.
A married couple, ages 60 and 58, had independently been using the same topical solution for years. She’d developed painful scarring from childbirth that made sex painful after menopause. He’d developed ED. Both resolved. And not through separate treatments. Through the same one.

The compound is DMSO, dimethyl sulfoxide, and there’s decades of laboratory evidence explaining why these stories keep repeating.
In isolated human erectile tissue, pre-contracted to simulate a flaccid state, DMSO produced dose-dependent relaxation starting at astonishingly low concentrations, and reached roughly 29% maximal relaxation on its own. At higher concentrations, it abolished the resting muscle tension entirely.
Because DMSO absorbs through skin so efficiently, those concentrations are reachable with simple topical use.

It gets more interesting when combined with other agents.
As a vehicle, DMSO potentiated Viagra’s effect on erectile tissue 16 to 80-fold. In men whose ED no longer responded to Viagra at all, DMSO still relaxed the tissue directly.
And testosterone dissolved in DMSO produced relaxation reaching 41 to 71%, far exceeding DMSO alone.

What makes this notable isn’t just erectile tissue.
DMSO also appears to resolve several of the conditions that cause ED in the first place.
In one study, vaginal DMSO measurably relaxed pelvic floor muscles on EMG, normalizing abnormal activity in 85% of patients. In men with chronic prostatitis, adding DMSO to treatment raised normal erectile function to 72.2%, compared to 41.1% in controls, alongside better clearance of infection and reduced inflammation.
Same compound. Different mechanism entirely. But the same outcome!

For Peyronie’s disease specifically, one protocol using topical DMSO across 66 men over 20 sessions found plaques shrank in 72.7% of cases, dissolved completely in 18.1%, and erectile function improved in 42.4%.
A separate long-term protocol saw 5 of 6 patients fully recover with no recurrence over two to four years.
This lines up with DMSO’s known ability to dissolve collagen and scar tissue, the exact material Peyronie’s plaques are made of.
Even genital herpes responded. In one account, four patients regained the ability to have intercourse after just two days of treatment.

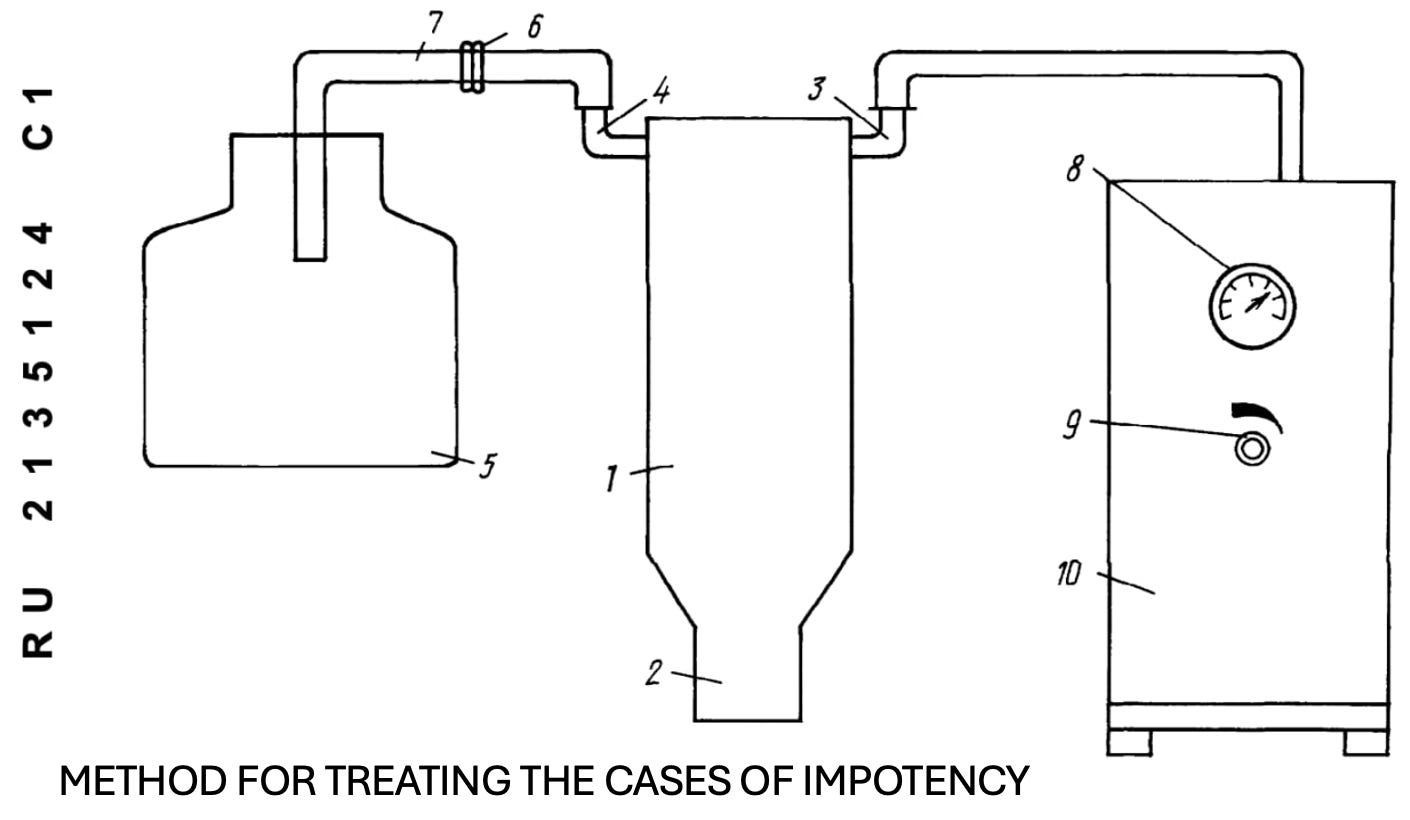
One of the more unusual approaches came from a Russian patent: DMSO mixed with papaverine, applied via a vacuum flask at controlled pressure and temperature, for 5 to 12 minutes per session over one to two weeks.
Every patient under 50 saw adequate restoration of erections. Among patients over 50, 72% did, and the rest still showed improvement.
The delivery method seems a bit strange. But it gets consistent results.
What’s striking isn’t any single result. It’s that one compound, acting through completely different mechanisms, resolves conditions medicine treats as entirely unrelated: vascular disease, nerve compression, scar tissue, chronic infection, hormonal collapse.
That’s not supposed to happen if these are truly separate diseases with separate causes.

The full article covers the exact DMSO protocols for treating ED directly, how Stanley Jacob enhanced its effect for Peyronie’s and Dupuytren’s, and how it’s used for broader urogenital issues in both men and women.
The Simple Ways to Restore Sexual Health
Medicine often carve the body into isolated parts and treat each one separately. A model like that is easy to standardize.
But when a single agent can resolve circulation problems, nerve dysfunction, scar tissue, and chronic infection, all conditions treated as unrelated, it suggests something the current model can’t quite account for: that circulation, nerves, connective tissue, and regeneration were never actually separate systems to begin with.
Until that’s taken seriously, a lot of men will keep being told their ED is simply something to live with. But it doesn’t have to be.
Thanks for reading! This information was based on a report originally published by A Midwestern Doctor. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
The Simple Ways to Restore Sexual Health
For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by A Midwestern Doctor:
How DMSO Heals The Nerves & Eliminates Pain
Exposing The Great Acid Reflux Scam
What’s The Healthiest Water To Drink?
While you’re at it, give A Midwestern Doctor a follow. No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed. This is easily one of the most valuable accounts you’ll ever follow.

If you haven’t subscribed to this Substack yet, take a moment to read what some of the most powerful voices in the medical freedom/truth movement have to say:
“The Vigilant Fox has been putting in a lot of work to create a news platform that shares the stories we want to hear about and brings attention to the most important things to know about. If you want a daily newsfeed in alignment with our ...”
– A Midwestern Doctor, The Forgotten Side of Medicine
“The Vigilant Fox absolutely is on top of things. We must support our fighters, and the Fox is fighting with truth.”
– Tom Renz, Tom Renz’s Newsletter
“Excellent capture of key video presentations on evolving pandemic science.”
– Peter A. McCullough, MD, MPH, FOCAL POINTS (Courageous Discourse)

Never had ED, but noticed many more morning pup tents taking supplement L’ Arginine (spelling error?)
The Midwestern Doctor is an Angel, perhaps 67 years old, and I won't tell, but maybe a woman? I bet she's "smoking hot" and a real "blast" to be around! Too bad I'm happily married to an amazing RN!!!! (The Magnificent Joy, Thai former head nurse at prominent hospital in BKK 23 years ago)! If the Midwestern Doctor is married? I bet he's quite a character! I don't socialize, (only close family). Midwestern Doc, without doxing yourself? (Don't do that!), are you within 125 miles of the windy city?
DMSO - healed me from the worst exposure I've ever had to poison ivy! Both legs, spread through sweat, before I knew what happened! DMSO was the only thing that worked! Using it on the topside of feet for minor neuropathy from a bad diet ending 13 years ago. 2 days, and it's working.
No issue with T, opposite since I'm 99% ketogenic. Midwestern Doc., if I get one vote, you're getting a full set of wings! Thanks for every piece of wisdom. Sainthood is next! I got some "pull"!