
The Forgotten TV Warning About Sleeping Pills and the Study That Linked Them to Death
It’s hard to believe this actually aired on TV.


The following information is based on a report originally published by A Midwestern Doctor. Key details have been streamlined and editorialized for clarity and impact. Read the original report here.
It’s hard to believe this ever made TV news.
But a sleeping pill study found you are “almost FIVE TIMES more likely to die [prematurely] if you pop the pills.”
“And at a certain dosage, 35% likelier to get cancer.”
“I don’t think there’s any dose which is safe,” said Dr. Daniel Kripke, one of the study’s leading researchers.
The local news reporter noted: “This is not the first study to associate sleeping pills with a higher rate for mortality. Eighteen other studies have also established the link.”
Sleeping pills “stop our brain cells from firing” to get us to sleep.
And if they can increase our risk of death, what are the other risks that no one is talking about?
Jordan Peterson disappeared from public view last year.
When his daughter finally broke her silence, her video got 10 million views in a matter of days. What she revealed: he was experiencing a devastating relapse from a previous benzodiazepine injury—triggered by stress and mold exposure.
Most people watching had never heard of anything like this. And some refused to believe it was possible.
But it is.
What she described is far more common than medicine will ever admit.
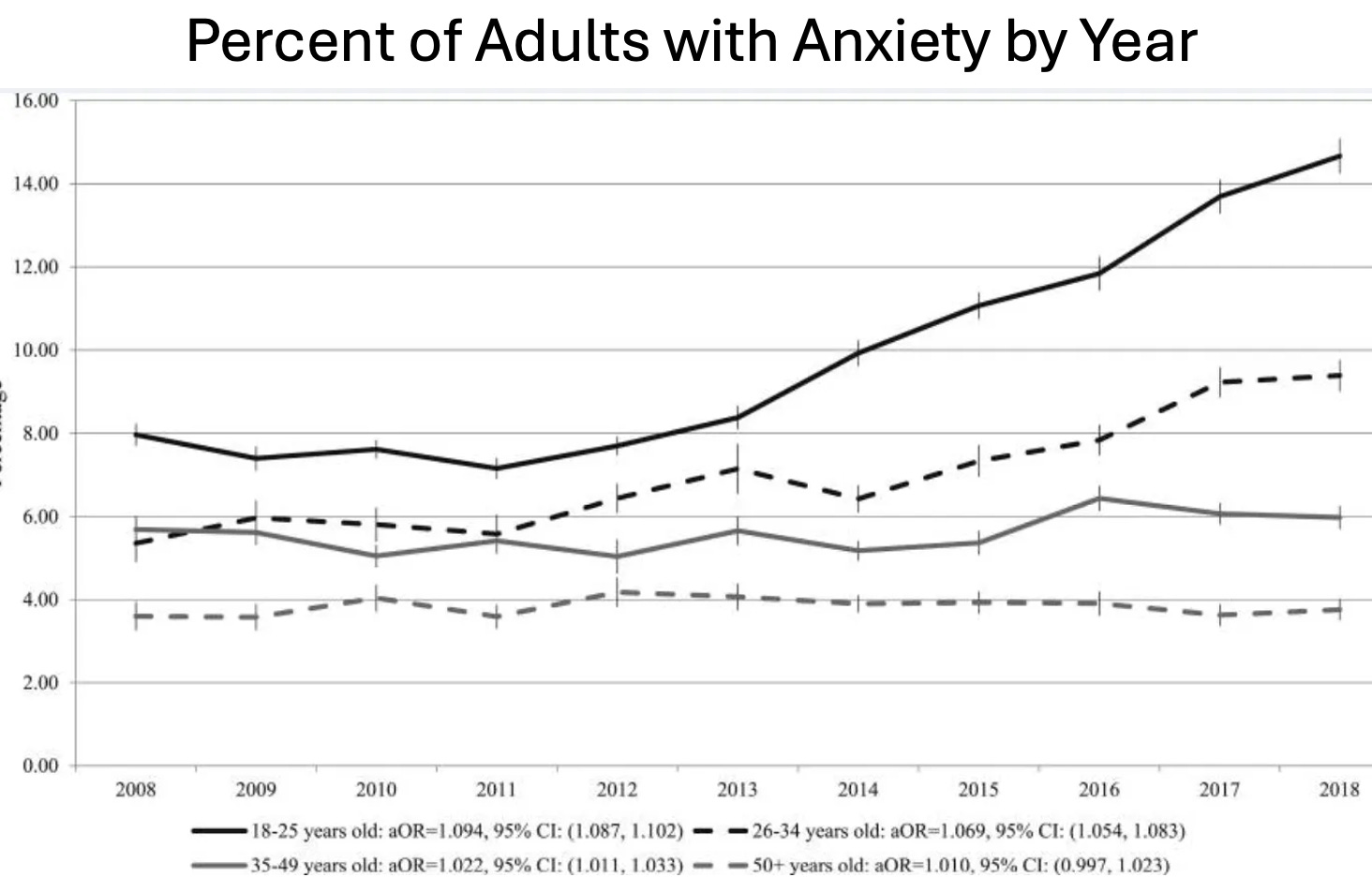
Anxiety is now the defining condition of modern life.
Take a moment to let that really sink in.
In the early 2000s, roughly 1 in 5 American adults had a diagnosable anxiety disorder. By 2023, more than half of young adults aged 18 to 26 reported suffering from anxiety. Forty-three percent had experienced panic attacks. A third were already on anxiety medications.
Despite spending $36.8 billion on anxiety and mood disorder care in 2007 alone, the problem has gotten measurably worse with every passing year.
That’s not a treatment failure. That’s a business model.
This information comes from the work of medical researcher A Midwestern Doctor. For all the sources and details, read the full report below.
What They Don’t Tell Us About Anxiety and Benzodiazepine Dangers

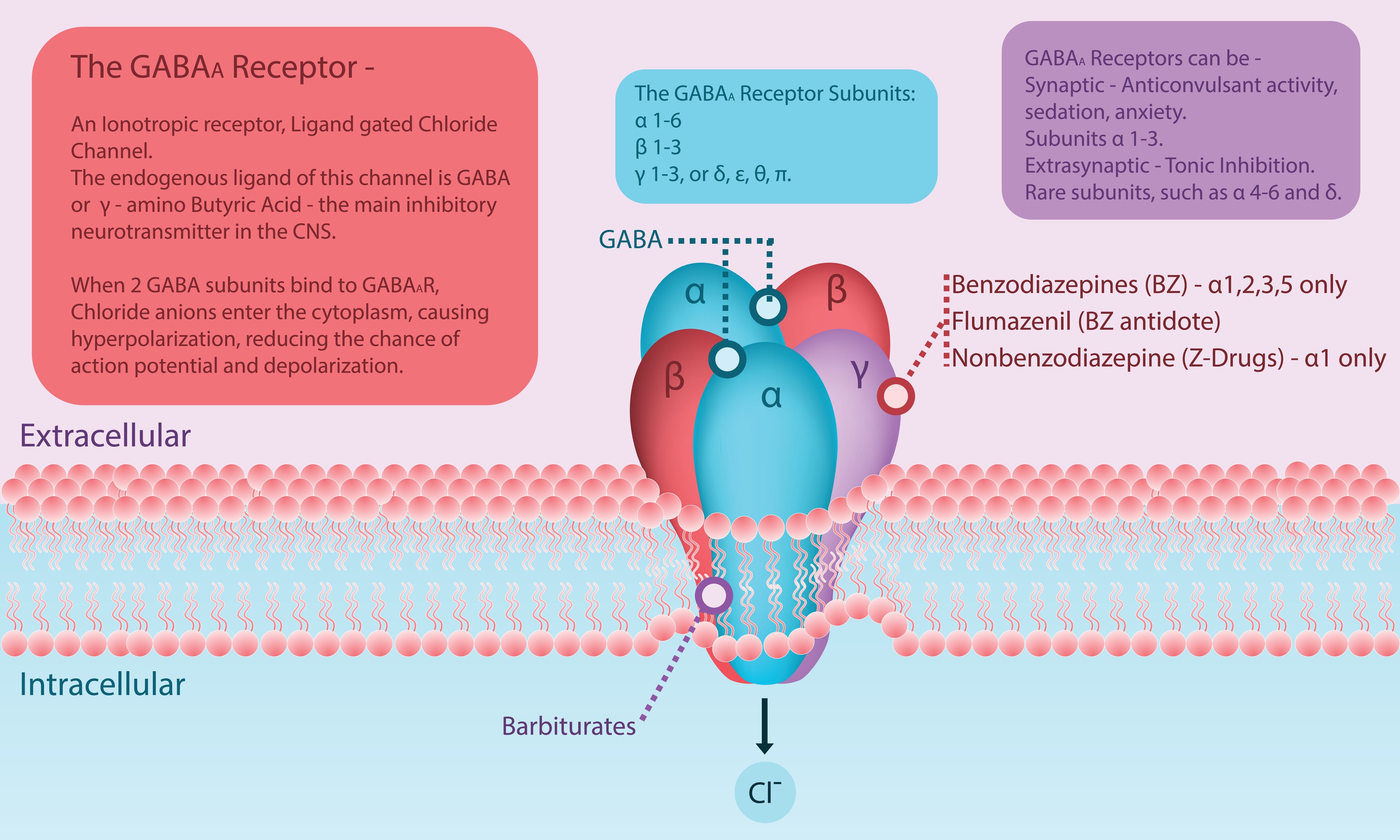
To understand why benzodiazepines are so dangerous, you have to understand what they do inside the brain.
The nervous system runs on a balance between stimulation and inhibition. The brain’s primary calming signal—its main inhibitory neurotransmitter—is called GABA. Alcohol, barbiturates, and benzodiazepines don’t directly activate GABA receptors. They amplify GABA’s effect on those receptors.
That distinction matters—a lot.
Here’s why. The brain constantly monitors its own receptor activity. When a receptor is being artificially overstimulated, the brain compensates by making it progressively harder to activate—a process called downregulation. This creates tolerance, which demands higher doses, which deepens the downregulation further.
When the drug is eventually stopped, those now-blunted GABA receptors can’t produce normal calming activity on their own no matter how much you want them to. What fills the void is called withdrawal.
And it can be catastrophic.
This is absolutely not a character flaw in the people that this happens to. It’s the predictable consequence of how the brain protects itself.
But that’s not how medicine responds to that consequence.
This isn’t the first time medicine has run this cycle.
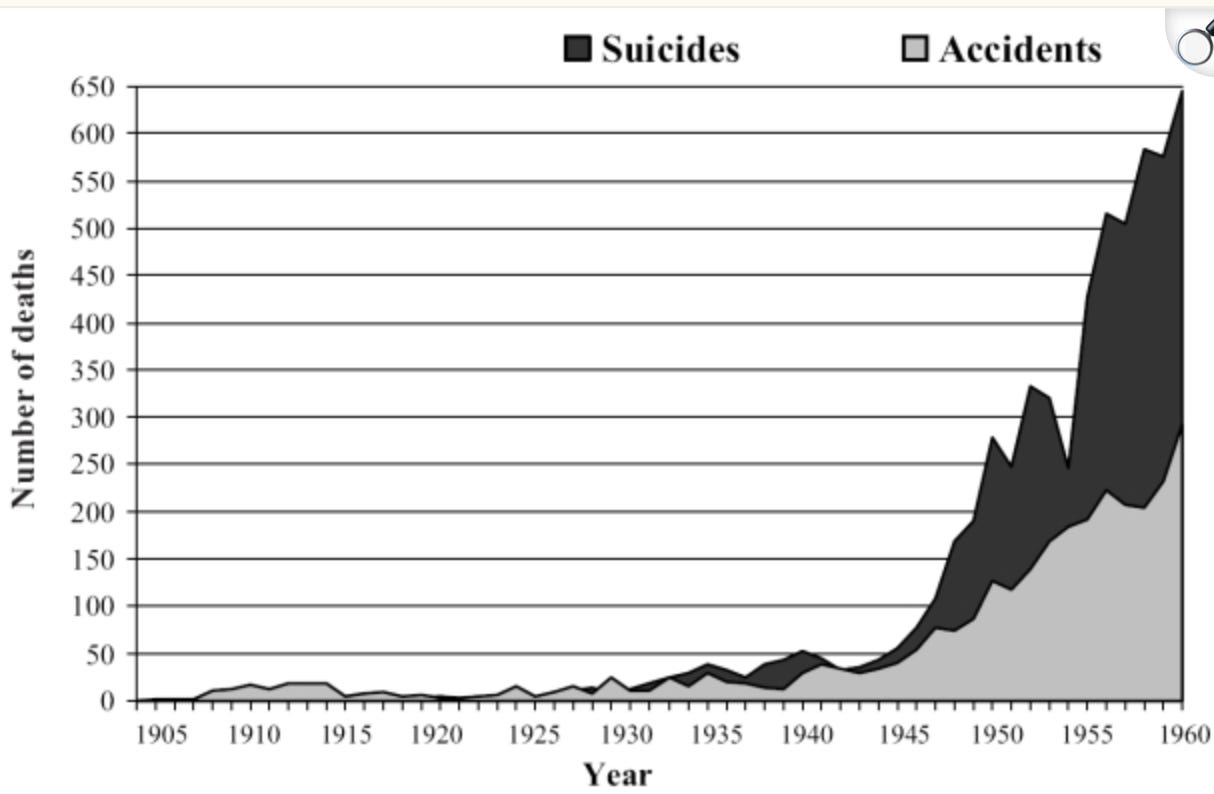
The first barbiturate was discovered way back in 1903. Within a year, medical literature was documenting the “Veronal habit.” But it took until the 1950s for reliable evidence of addiction to accumulate, and until the 1970s for laws restricting their use. That’s a long time.
By 1962, Kennedy’s commission estimated 250,000 Americans were addicted to barbiturates. England had 135,000. Among the overdose deaths: Marilyn Monroe.
The barbiturates weren’t restricted because the evidence finally became undeniable. They were restricted when a replacement was ready.
A Midwestern Doctor traces the exact playbook used to bring benzodiazepines to market—including who ran the marketing campaign, how they kept the most addicted patients out of the FDA trial, and why they targeted general practitioners instead of psychiatrists.
What They Don’t Tell Us About Anxiety and Benzodiazepine Dangers
When barbiturates became a liability, pharmaceutical companies went looking for a safer alternative. One Roche researcher pursued the problem for years—even after being ordered to stop. In 1956, he found what would become the first benzodiazepine.
Roche recognized immediately it would be a blockbuster.
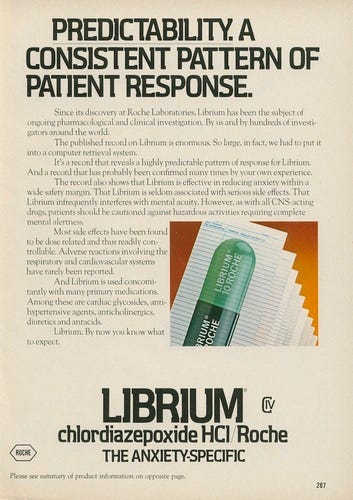
To get FDA approval, they ran one of the largest clinical trials in history: roughly 20,000 patients. Then they selected 1,163 of them—specifically those who showed no signs of addiction or tolerance—and presented only those results to the FDA.
That cherry-picked dataset won the 1960 approval for Librium.
Roche then hired Arthur Sackler to run the marketing campaign. Sackler arranged for newspapers nationwide to publish favorable stories, placed those publications in doctors’ offices (bypassing advertising regulations), aggressively targeted women’s magazines, and deliberately went after general practitioners rather than psychiatrists—because GPs were far less likely to recognize the drug’s dangers. Psychiatrists already knew what sedatives could do.
Yikes.
By 1963, the follow-up campaign for Valium was underway. Both were, by any measure, extraordinarily successful.
In its first month on the market, Librium generated 1.5 million prescriptions.
It was dispensed for everything under the sun—anxiety, phobias, high blood pressure, ulcers, acne, muscle pain, and headaches.
Even John Kennedy—struggling with back pain from wartime injuries—took it.
By the mid-1970s, benzodiazepines topped every “most frequently prescribed” list in American medicine.
The campaign used to sell Librium and Valium—market a drug as safe and non-addictive, target doctors unlikely to recognize the danger, frame an almost unlimited condition as undertreated—became a template.
Arthur Sackler’s descendants used the same playbook with synthetic opioids. And we all know how that turned out.
Benzodiazepines are now losing their institutional defenders primarily because they’ve gone off-patent. With no financial incentive left to protect them, the consensus is finally beginning to shift.
And that tells you something about where the consensus came from in the first place.
Benzodiazepines cause harm in three distinct, well-documented categories.
Each one is serious on its own. Together, they explain how millions of people who never intended to become dependent ended up trapped for years—some for decades—by a drug their doctor prescribed for anxiety.
Here’s what they actually do:

The first harm is one almost no one is told about: benzodiazepines don’t put you to sleep. They sedate you.
Sedation is not restorative sleep. When benzos suppress the nervous system, they simultaneously block the deep stages of sleep your brain requires to function. Patients who believe they’re finally resting are, physiologically, experiencing all the consequences of chronic sleep deprivation.
Studies have found sleeping pill users are two to five times as likely to die as non-users. One estimate concluded that prescription sleeping pills may have been associated with 320,000 to 507,000 excess deaths in the United States in a single year.
That’s not a side effect. That’s a central feature of how these drugs work.

The second category of harm is what benzos do to the brain over time.
Long-term use creates measurable impairment in processing speed, working memory, sustained attention, and the formation of new memories. About 20.7% of long-term users show cognitive deficits across multiple domains.
Meta-analyses find that long-term use increases the risk of dementia by 51%. That’s huge.
One study documented that in the first three years of use, benzodiazepines create driving impairment exceeding the legal alcohol limit for a DUI. A large study of nursing home residents found benzos increase the risk of falls by 44%. Long-acting benzos increase car accident risk by 45% overall. Commercial drivers are actually legally prohibited from taking them.
There’s also the memory effect many long-term users describe: time moving strangely fast, a dreamlike flow state, an inability to recall what was happening during the years they were on the drug—a phenomenon called anterograde amnesia. Research from 1972 found that regular diazepam doses reduced recognition memory in 90% of women.
The people prescribing these drugs often meet the patient for 15 minutes.
One of the most dispiriting data points in A Midwestern Doctor’s article: a 1979 Senate hearing put the benzo problem on public record—44 million Valium prescriptions, documented dependence, a manufacturer insisting it was safe.
Wait until you see what happened to prescribing rates in the decades that followed.
What They Don’t Tell Us About Anxiety and Benzodiazepine Dangers
Roughly half of all benzodiazepine users experience withdrawal symptoms when they stop or reduce their dose.
About 20 to 30 percent experience rebound—their original symptoms return worse than before they ever started the drug. Around 10 percent go through withdrawals severe enough to be “quite distressing,” and those individuals are 40% more likely to become suicidal during that period.
People who discontinued benzos in one study were found to be 60% more likely to die in the following year.
Tapering takes years.
Doing it too quickly, even slightly, can trigger a backlash that makes stopping even harder.

When benzodiazepines wear off, they don’t simply stop working. The GABA system has been progressively suppressed, and what rebounds mirrors alcohol withdrawal in severity.
Common symptoms include anxiety, insomnia, panic attacks, tremors, heart palpitations, and sweating. Psychological symptoms include confusion, memory problems, hallucinations, paranoia, and depression. Sensory symptoms include tinnitus and a dissociative detachment from reality—a feeling of not quite inhabiting your own life. In the most severe cases: seizures. Which without treatment can be fatal.
For 10 to 15 percent of users, post-acute withdrawal symptoms—anxiety, cognitive impairment, depression, sleep disruption—persist for months to years.
Typically one to two years.
In some cases, five to ten.
Using benzodiazepines for as little as three to six weeks can create the physical dependence that leads to all of this.
Most patients were never told that.

This was all documented publicly in 1979.
At a Senate subcommittee hearing chaired by Senator Edward Kennedy, a Navy psychiatrist testified that patients were becoming addicted to Valium in as little as six weeks. More than 44.6 million Valium prescriptions had been written that year. Kennedy called it a “nightmare of dependence.”
“None of these drugs solve our problems,” the psychiatrist testified. “They make people feel better because they make you feel dull and insensitive.”
The manufacturer of Valium—Hoffmann-La Roche—responded that addiction was “extremely rare” at recommended dosages.
That exchange happened 47 years ago.

After that Senate hearing, benzodiazepine use didn’t decline. It accelerated.
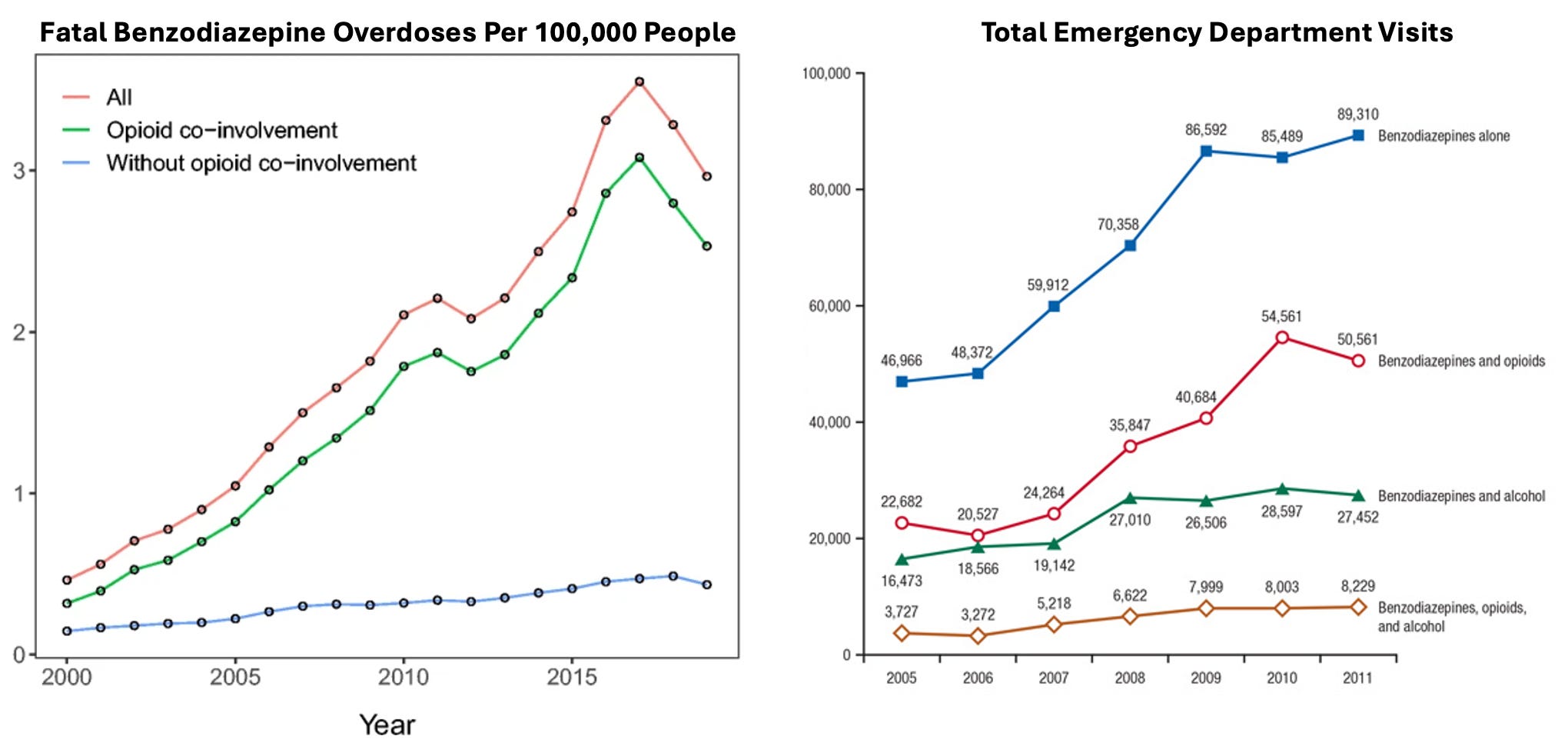
In 1996, 4.1% of American adults had a benzodiazepine prescription. By 2018, 12.6% reported benzo use in the past year. Emergency room visits involving benzo misuse rose 149% between 2004 and 2011.
Overdose deaths climbed from 1,135 in 1999 to 12,499 in 2021.
That’s a 917% increase in 22 years.
Michael Jackson. Heath Ledger. Tom Petty. Prince.
Each of these deaths involved benzodiazepines.
None are fringe cases.
They represent a fraction of the roughly 12,500 people who died from benzo overdoses in 2021 alone.

There’s a structural reason this crisis keeps escalating, and it’s built into the architecture of modern medicine itself.
Appropriate benzodiazepine prescribing requires understanding which specific type of anxiety a patient has, whether benzos are even indicated for that type, what the risks are given the patient’s age and other medications, how to taper appropriately, and how to monitor for dependence over time.
It’s clear as day that none of that is possible in a 15-minute insurance-reimbursed visit.
Many patients were never warned that dependence can develop in only three to six weeks—and that once it does, stopping may be impossible without a years-long tapering process. And many were never told that going even slightly too fast creates a backlash that makes quitting harder.
People end up on benzodiazepines for decades, for conditions the drugs are actively worsening.
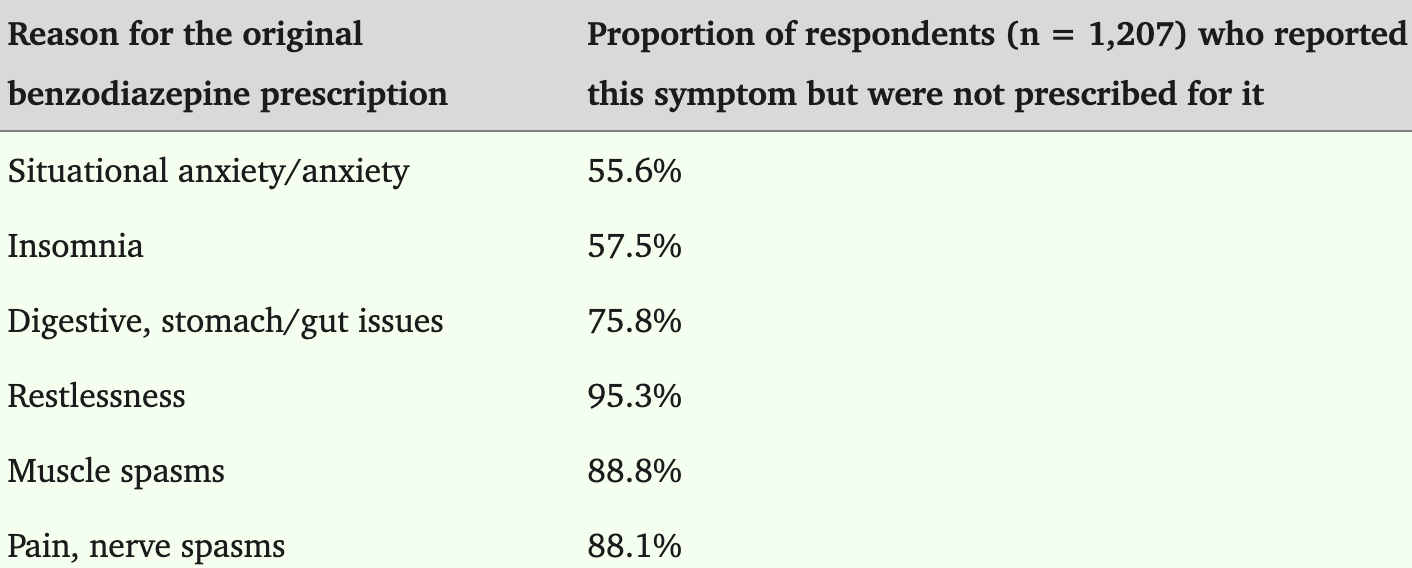
A survey of 1,207 benzo users found that 95.3% of those originally prescribed for restlessness developed restlessness as a new drug-induced symptom. For anxiety: 55.6%. For insomnia: 57.5%.
The drug was creating the very problem it was prescribed to treat.
Here’s what almost never gets addressed: anxiety isn’t one disease.
Multiple distinct types exist, each with different root causes and different responses to treatment.
Giving the same medication to all of them makes about as much sense as treating every patient with chest pain identically.
In some cases, benzodiazepines are genuinely appropriate. In others, they make the underlying condition measurably worse.
15 minutes is not enough time to figure that out.

Generalized anxiety disorder often worsens with benzodiazepines, requiring progressively higher doses over time. Cognitive behavioral therapy is far more effective here—and the research supports it clearly.
But panic disorder is different. When panic attacks have a warning symptom before they begin, benzos taken at that moment can be genuinely useful. Without that warning symptom there is minimal benefit.
OCD doesn’t respond to CBT or benzodiazepines at all. It responds to a different therapeutic model entirely.
Social anxiety disorder typically responds best to low-dose beta-blockers rather than habit-forming sedatives.
The 15-minute visit treats all of these as one condition.

What’s driving the anxiety epidemic isn’t purely psychological.
Autonomic nervous system imbalances, reactive hypoglycemia, circadian disruption from artificial light, thyroid disorders, cardiovascular conditions—each of these can manifest as anxiety.
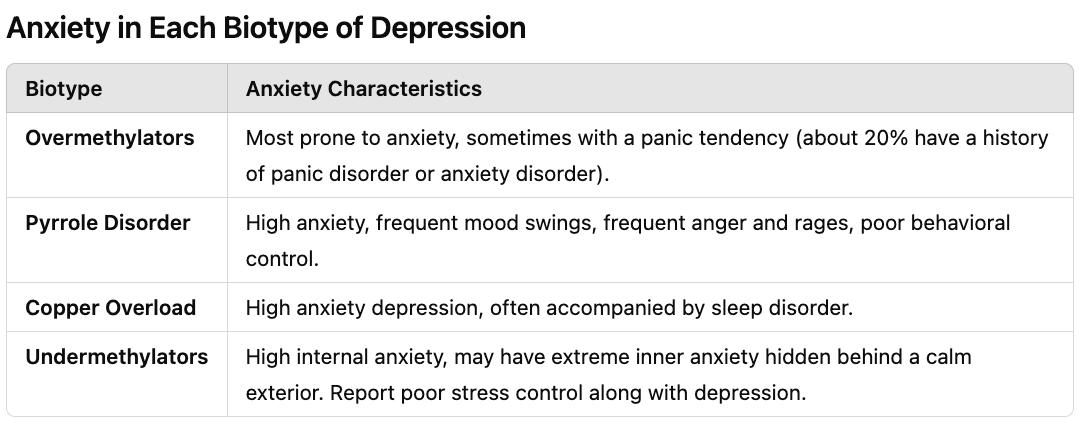
Research on the blood chemistry of 2,800 individuals identified five distinct metabolic patterns underlying depression and anxiety, each with its own treatment profile and its own response to benzodiazepines.
The underlying causes of anxiety are rarely identified in conventional care. When the root cause is left untreated and only the symptom is managed pharmacologically, the condition doesn’t resolve—it deepens.
And the drug prescribed to manage it often accelerates that process.
The subscriber-only section of A Midwestern Doctor’s article covers what actually works: specific supplements, natural therapies, appropriate non-benzo anxiety medications, psychedelic-assisted psychotherapy, mind-body approaches, and detailed strategies for withdrawing from benzodiazepines.
If you or someone you know is on benzos, that section alone is worth subscribing.
What They Don’t Tell Us About Anxiety and Benzodiazepine Dangers
There’s a pattern that runs through the entire history of pharmaceutical sedatives that’s worth spending some extra time on.
Barbiturates were documented as addictive within a year of hitting the market—but concerns were suppressed until a replacement was ready. Librium was marketed as safe while cherry-picked trial data won FDA approval and the same marketing family that would later fuel the opioid crisis ran the campaign. A Senate hearing documented a “nightmare of dependence” with 44 million prescriptions—and the manufacturer called addiction “extremely rare.” Prescriptions tripled over the following four decades.
More than 1 in 8 American adults took a benzodiazepine last year. 12,499 people died from benzo overdoses in 2021.
None of this persisted because of ignorance. The knowledge was there. The Senate hearing was on record. The mechanisms were understood. What kept the system in place was that anxious people are a reliable, renewable market—and the most reliable way to keep that market intact is to treat the symptom without ever touching the cause.
The most unsettling part isn’t that this happened. It’s that it’s still happening—and the same structural incentives that drove it are still in place.
When the most common response to human suffering is a drug that produces the very condition it was prescribed to treat, that isn’t medicine failing. That’s something else entirely—and we haven’t yet had an honest reckoning with what it is.

Thanks for reading! This information was based on a report originally published by A Midwestern Doctor. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
What They Don’t Tell Us About Anxiety and Benzodiazepine Dangers
For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by A Midwestern Doctor:
We Now Know How The Government Lied About the COVID Vaccines
The Hidden Dangers of Hospital Births & How to Protect Your Family
What’s The Healthiest Water To Drink?
While you’re at it, give A Midwestern Doctor a follow. No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed. This is easily one of the most valuable accounts you’ll ever follow.

If you haven’t subscribed to this Substack yet, take a moment to read what some of the most powerful voices in the medical freedom/truth movement have to say:
“The Vigilant Fox has been putting in a lot of work to create a news platform that shares the stories we want to hear about and brings attention to the most important things to know about. If you want a daily newsfeed in alignment with our ...”
– A Midwestern Doctor, The Forgotten Side of Medicine
“The Vigilant Fox absolutely is on top of things. We must support our fighters, and the Fox is fighting with truth.”
– Tom Renz, Tom Renz’s Newsletter
“Excellent capture of key video presentations on evolving pandemic science.”
– Peter A. McCullough, MD, MPH, FOCAL POINTS (Courageous Discourse)

Human arrogance… Somehow, people bought into the myth that natural feelings are illnesses and if you are “sick,” whatever your problem is, you must take some synthetic chemical. As the article also observes, the body can get used to a synthetic replacement of something it normally produces. It happens for “high blood pressure” and “high blood sugar” all the time. Ironically, diabetes can qualify as an “infection” and the same can happen to “psychiatric disorders.”
https://rayhorvaththesource.substack.com/p/what-has-been-causing-the-astronomical
Increasing levels of wireless radiation of all kinds can ID, track, and target a person, and they can converge:
https://rayhorvaththesource.substack.com/p/the-slow-and-invisible-killers
“Doctors” cautiously avoid the options and ignore areal radiation and toxic exposure, too. They prefer to say, it’s a “genetic” disorder, while the DNA/RNA model has never been proven, and only seems to be a cover story for something else:
https://rayhorvaththesource.substack.com/p/how-is-life-encoded
Between 1910-1920 the Rockefeller Foundation funded reforms at several prominent medical schools, including Washington University at St. Louis, Yale University, the University of Chicago, and Vanderbilt University. These reforms established a single high standard for medical education in the U.S. which resulted in influence of wealthy donors, particularly John D. Rockefeller, on medical education in the US.
8n 1913 Abraham Flexner (who had no nedical education) was hired by the Rockefellar Foundation to advise its General Education Board which marked the beginning of systematic funding for reforms at various medical schools. The Carnegie Foundation was very envolved as well.
Philanthropic funding from the Rockefeller and Carnegie Foundations helped to standardize medical education, ensuring that schools adhered to higher educational standards and evidence based science practices which were needed.
The problem was that the reforms promoted allopathic medicine, dependence on use of pharmaceuticals to treat disease, which became the dominant form of medical practice, sidelining other healing modalities like homeopathy, naturopathy, osteopathy, eastern medicine, ect.
Rockefeller’s influence didn’t stop at medical education. In 1901, he established the Rockefeller Institute for Medical Research (now Rockefeller University), a center dedicated to advancing biomedical research. The institute was instrumental in pioneering various medical treatments, including vaccines, antibiotics, and synthetic drugs, which would become the cornerstones of the burgeoning pharmaceutical industry.
Rockefeller's strategy was clear: focus on pharmaceutical-based treatments rather than natural or holistic approaches. This focus aligned with his business interests, particularly in the chemical industry, which provided the raw materials for many of the drugs being developed. By promoting a pharmaceutical-centered approach to medicine, Rockefeller helped create a market for chemical-based treatments, establishing a system in which drugs, rather than preventive or holistic care, became the primary method of addressing health issues
The reforms negatively impacted the ethos of medicine in its blind passion for science and education by aligning too much with the pharmaceutical industry's vaccines, antibiotics, and synthetic drugs, making medicine and medication about profit not people, and turning their backs on alternative modalities for treatment of disease and the use natural substances rather than a pharmaceutical synthetic drugs.
What was the cost of success, and who has borne that burden? Review of medical care in the last century documents that the trust and respect that were extended to the medical profession 50 years ago have been substantially eroded. There has been a fall from grace of the vaunted medical profession. Physicians have lost their authenticity as trusted healers. In the end, I believe its the billions of Patients receiving the medical treatment and the pharmaceutical drugs that have ended up paying the highest price...