
Journal Hit by Cyberattacks After Publishing COVID “Vaccine” Cancer Study
Someone clearly didn’t want this data circulating.
This article originally appeared on Focal Points and was republished with permission.
Guest post by Nicolas Hulscher, MPH
For several years now, clinicians, pathologists, and independent researchers have been documenting turbo cancers following COVID-19 vaccination: sudden relapses, explosive disease acceleration, rare malignancies appearing out of nowhere, and tumors localizing to injection sites or draining lymph nodes. These signals have been visible for some time — but deliberately fragmented, dismissed as coincidence, or buried under claims that “case reports don’t count.”
That excuse has now completely collapsed.
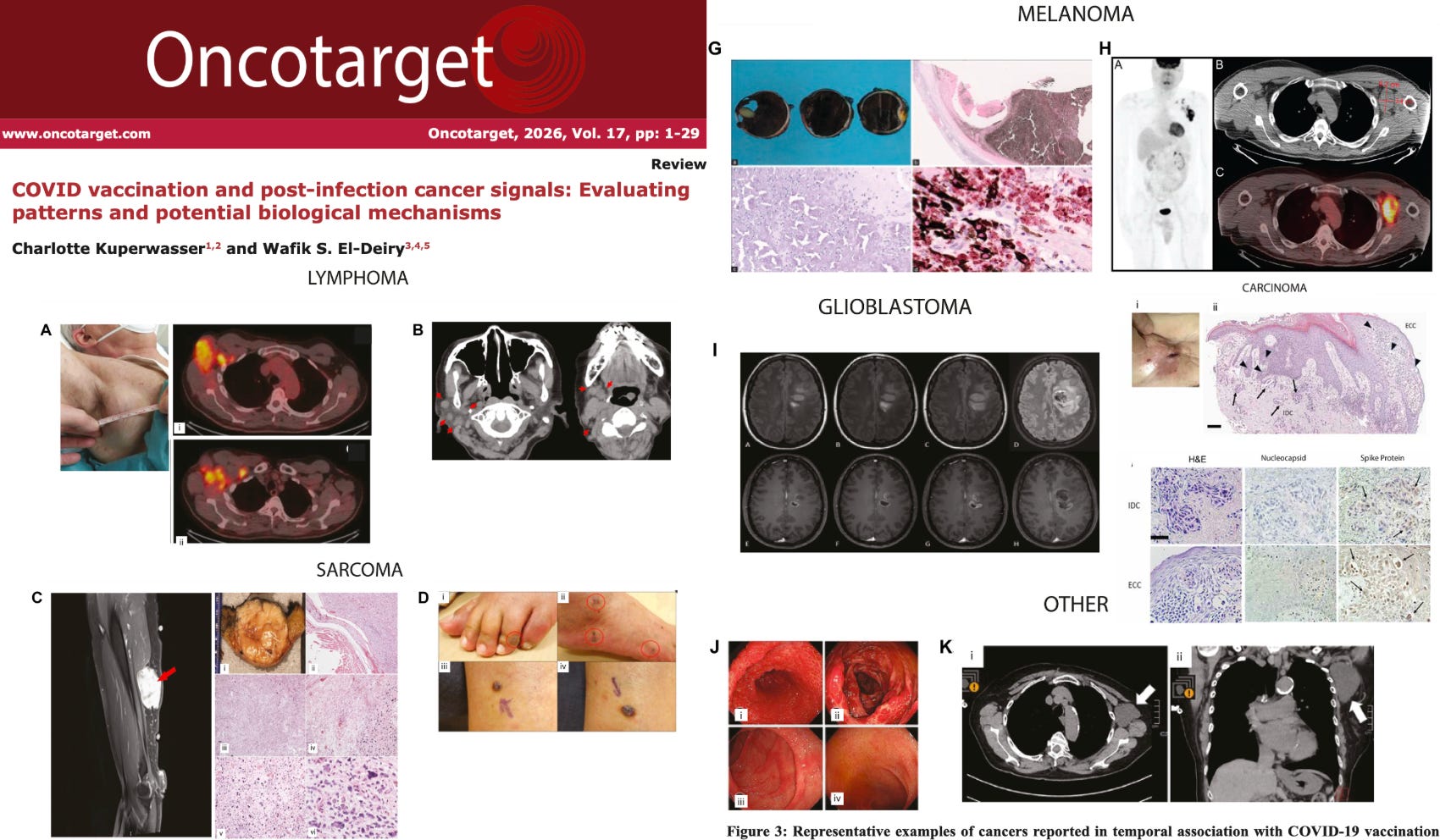
A newly published peer-reviewed systematic review in Oncotarget — authored by Charlotte Kuperwasser, PhD, and Wafik S. El-Deiry, MD, PhD — is the first to formally assemble and analyze the entire published literature on cancer temporally associated with COVID-19 vaccination and SARS-CoV-2 infection.
Importantly, while this article has been accepted, published, and assigned a publication date, the journal has disclosed that it is currently unable to add the paper to its live journal index due to an ongoing malicious cyberattack on its servers.



According to a statement now posted on Oncotarget’s website — and relayed directly to us by Dr. El-Deiry — the journal experienced sustained cyber intrusions in December 2025 and January 2026, which were reported to the FBI, with attacks continuing into the present. In the meantime, Dr. El-Deiry has provided a link to access this important paper. You can read it here.

The journal further states that it is investigating whether individuals associated with PubPeer (PubSmear Mob) may have engaged in or facilitated cybercriminal activity, including server hacking, taking journal websites offline, and manipulating Google search results to suppress journals and scientists. Oncotarget reports that it is currently in contact with federal law-enforcement agencies regarding identified suspects.
The authors conducted a global, multi-database search (PubMed, Scopus, Web of Science, Google Scholar, React19) covering January 2020 through October 2025, explicitly hunting for cancer diagnoses, recurrences, or aggressive progression following vaccination or infection.
What they ultimately identified is not trivial:
69 peer-reviewed publications
333 individual cancer cases
27 countries
66 article-level case reports and series
2 large population-level cohort studies
1 longitudinal U.S. military cancer surveillance analysis
Multiple mechanistic and translational studies
Taken together, this constitutes the most comprehensive oncologic safety assessment related to COVID-19 vaccination published to date.
Cancer Types
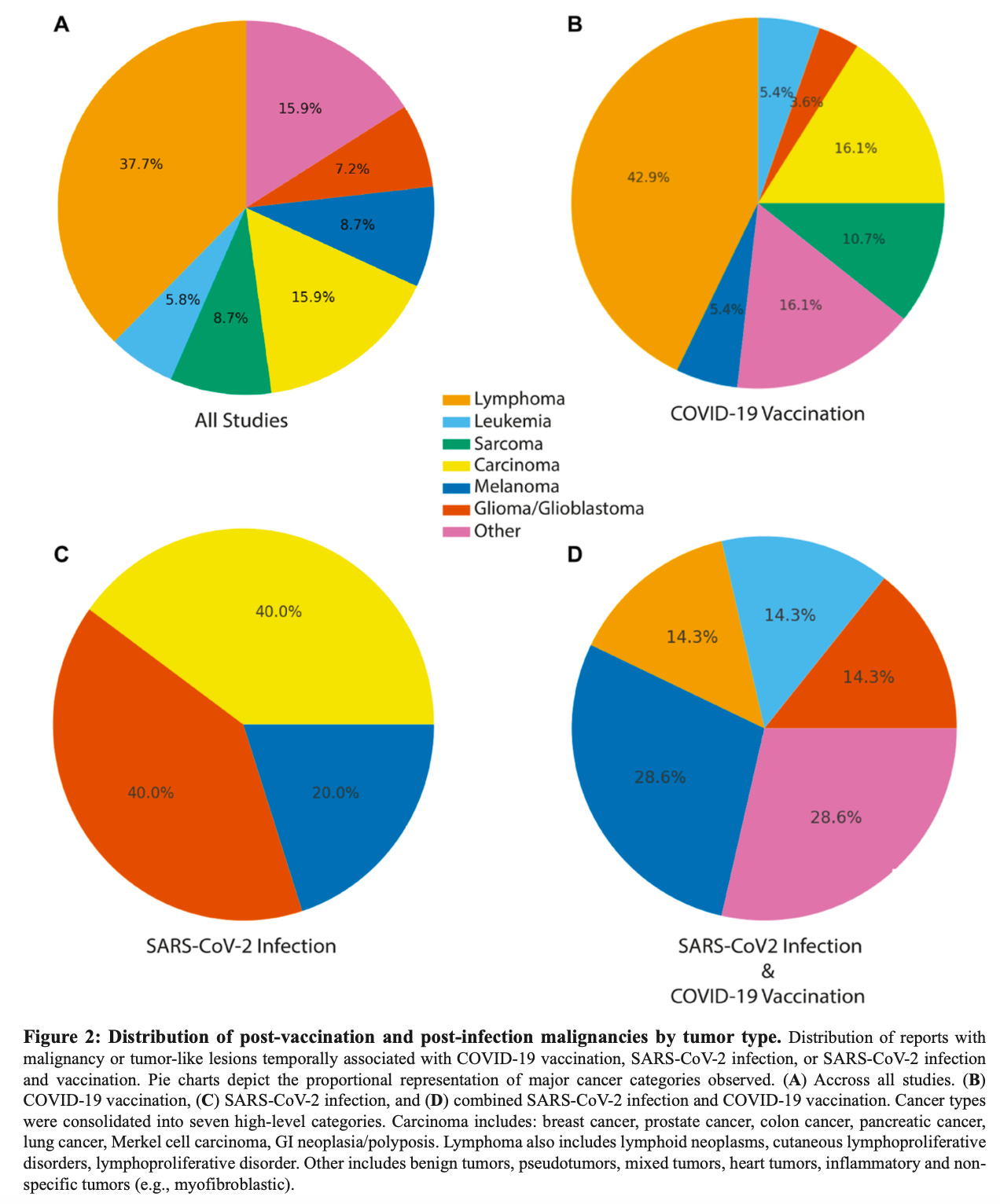
Across all 66 case reports/case series (333 cancer cases), cancers were distributed as follows:
Lymphoma: ~38%
Carcinoma: ~16%
Other tumors: ~16%
Melanoma: ~9%
Sarcoma: ~9%
Glioma/Glioblastoma: ~7%
Leukemia: ~6%
Among COVID-19 vaccination–associated cases, lymphoid malignancies were even more prominent:
Lymphoma: ~43%
Carcinoma: ~16%
Sarcoma: ~11%
Other tumors: ~16%
Melanoma: ~5%
Glioma/Glioblastoma: ~4%
Leukemia: ~5%
SARS-CoV-2 infection–only cases were rare and showed a limited tumor spectrum:
Carcinoma: ~40%
Glioma/Glioblastoma: ~40%
Melanoma: ~20%
Cases involving both SARS-CoV-2 infection and COVID-19 vaccination showed a broader distribution:
Melanoma: ~29%
Other tumors: ~29%
Lymphoma: ~14%
Leukemia: ~14%
Glioma/Glioblastoma: ~14%
Overall, this demonstrates that vaccination-associated reports dominate the dataset, while infection-only cancer reports are comparatively few, and that lymphoid malignancies account for the largest proportion of cases, particularly in the vaccination-associated group.
Vaccine Platforms
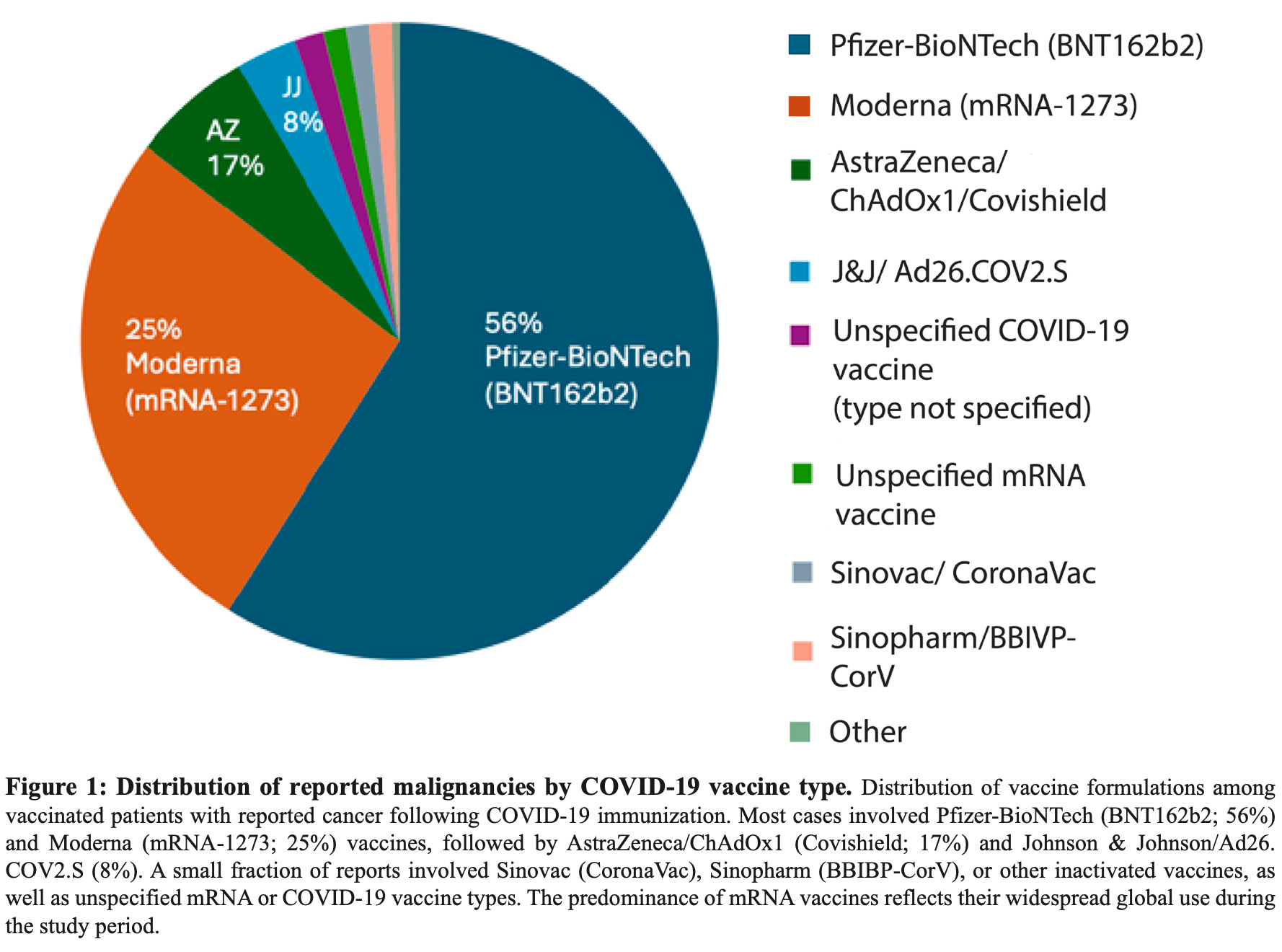
Among vaccination-associated cancer reports, mRNA injections account for the majority of cases, followed by adenoviral vector platforms, with inactivated vaccines reported infrequently.
Pfizer–BioNTech (BNT162b2): ~56%
Moderna (mRNA-1273): ~25%
AstraZeneca / ChAdOx1 (Covishield): ~17%
Johnson & Johnson / Ad26.COV2.S: ~8%
Unspecified COVID-19 vaccine type: small fraction
Unspecified mRNA vaccine: small fraction
Inactivated vaccines (Sinovac/CoronaVac, Sinopharm/BBIBP-CorV): rare
Other vaccine platforms: rare
Overall, the figure shows that reported malignancies are predominantly associated with mRNA vaccine platforms, with adenoviral vector vaccines contributing a smaller but notable share, and inactivated vaccines comprising only a minimal proportion of reports.
Temporality
Across the 333 cancer cases:
~50% of cases occurred within 2–4 weeks of vaccination
Some appeared within 7–14 days
Others emerged over 2–6 months or longer
Several underlying studies reported mean onset intervals of ~8–9 weeks
Importantly, many events followed second doses or boosters, pointing toward cumulative immune disruption. These timelines are entirely consistent with tumor promotion, immune escape, or reactivation of dormant disease, not de novo cancer initiation alone. The debunking method that “cancer takes decades” is no longer defensible.
Population-Level Evidence Supports the Clinical Signal
Beyond individual case reports, the authors also identified three large population-scale analyses that independently align with the observed clinical patterns.
South Korea (≈8.4 million individuals):
A nationwide cohort analysis identified statistically significant associations between COVID-19 vaccination and multiple cancer types, including thyroid, colorectal, lung, breast, and prostate cancers. Associations varied by vaccine platform, cumulative dose, age, and sex, indicating heterogeneity rather than a uniform background effect.Italy (≈300,000 individuals):
A population-based study found higher cancer hospitalization rates among vaccinated individuals, with the strongest signals observed at shorter latency intervals following vaccination.U.S. military (≈1.3 million service members):
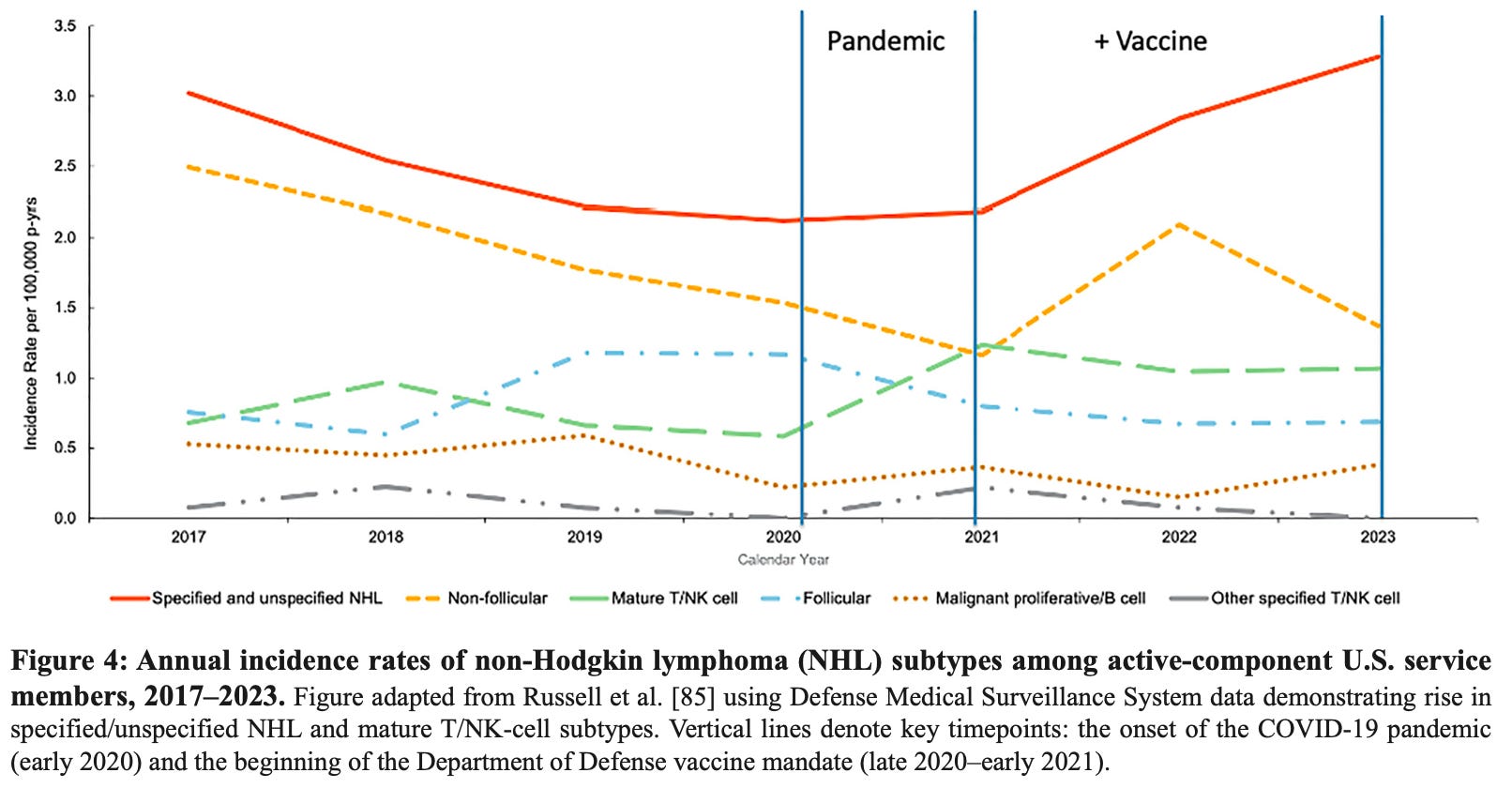
Longitudinal surveillance data documented a post-2021 increase in T/NK-cell lymphomas coinciding with the transition from the pre-pandemic period to near-universal COVID-19 vaccination in this highly structured population.
Biological Mechanisms
The review identifies three converging biological mechanisms that plausibly explain the observed cancer patterns following COVID-19 vaccination.
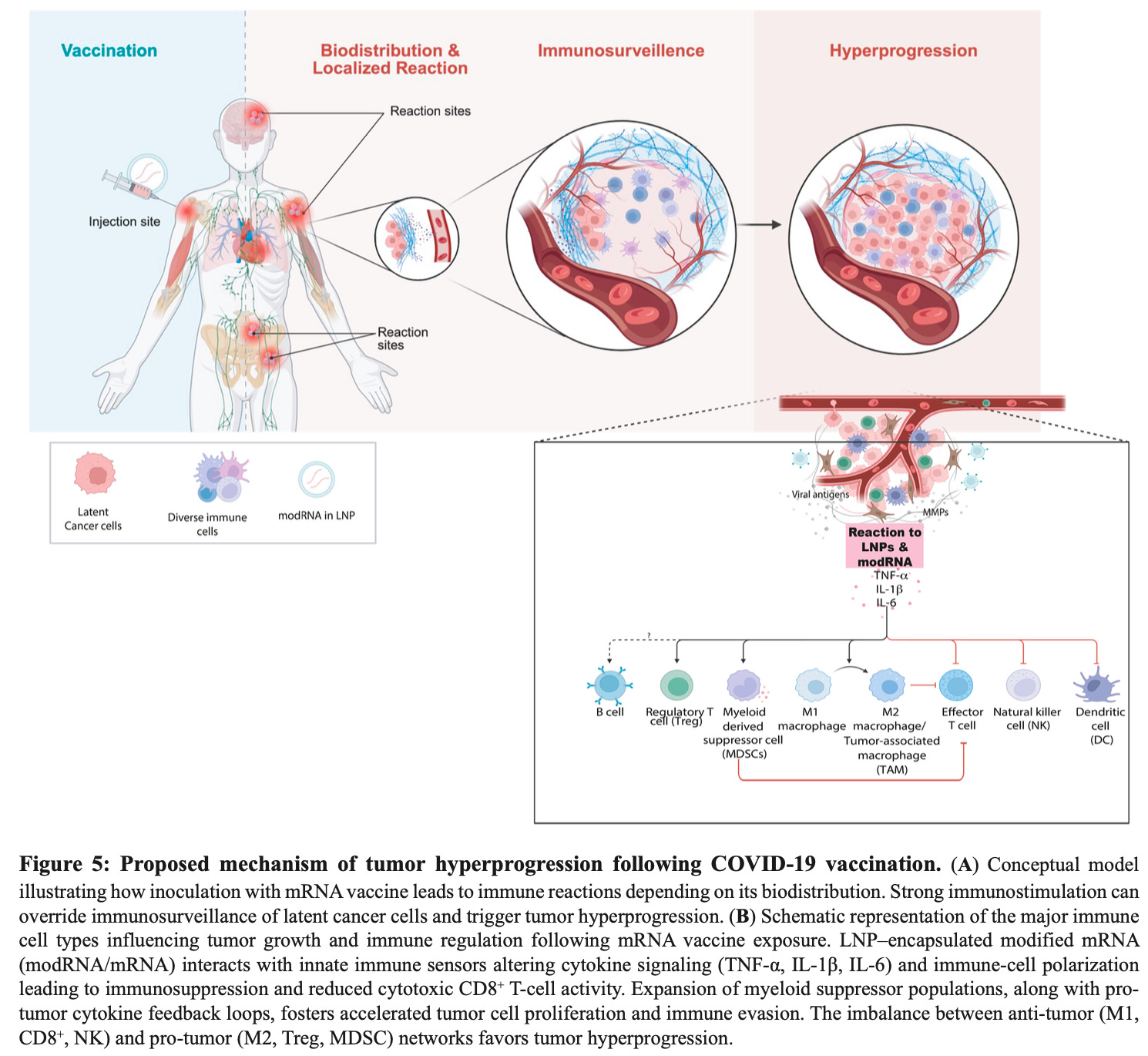
Immune dysregulation and loss of tumor surveillance.
Figure 5 illustrates how lipid nanoparticle–encapsulated mRNA can trigger strong localized and systemic immune activation, including cytokine release (TNF-α, IL-1β, IL-6). This immune shift reduces cytotoxic CD8⁺ T-cell and NK-cell activity while expanding immunosuppressive populations (Tregs, MDSCs, M2 macrophages), creating conditions that allow latent or controlled tumors to escape immune surveillance and rapidly progress.
Spike protein persistence and tumor-promoting effects.
Vaccine-derived spike protein can persist for months to years, disrupt tumor-suppressor pathways, induce DNA damage responses, and has been detected within tumor tissue without nucleocapsid protein, confirming vaccine origin. Persistent spike exposure within the tumor microenvironment can promote angiogenesis, immune evasion, and accelerated growth.
Residual DNA contaminants.
Independent analyses have identified plasmid DNA fragments, including SV40 regulatory elements, encapsulated within lipid nanoparticles. This delivery system enhances cellular uptake and raises concerns about genomic interaction and prolonged immune activation, further tipping the balance toward tumor hyperprogression.
These mechanisms converge to shift the immune system from tumor control to tumor promotion, favoring rapid progression and immune escape — risks that were never adequately evaluated prior to mass deployment.
Conclusion
For the first time, a major cancer journal has consolidated what many clinicians, pathologists, and researchers have already recognized and placed it permanently into the peer-reviewed scientific record. At this point, continued refusal by federal health agencies to acknowledge these signals represents criminal negligence.
Equally grave are the journal’s public disclosures that its servers were subjected to malicious cyberattacks possibly linked to PubPeer members, which have interfered with access to this published study. The suppression or obstruction of peer-reviewed cancer safety data through cybercrime is deeply worrisome and warrants federal action.
Those responsible for cybercriminal interference will ultimately be held accountable — and regulators who ignored or suppressed post-vaccination cancer signals cannot escape responsibility for the human consequences. Every preventable post-vaccination cancer now rests squarely with regulatory authorities who ignored, dismissed, or suppressed clear safety warnings.
Epidemiologist and Foundation Administrator, McCullough Foundation
www.mcculloughfnd.org
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
Copyright 2026 Focal Points
