
“Conspiracy Theory” No More: The Truth About COVID Vaccine Shedding
The evidence shows that shedding from the COVID jab isn’t just real. It’s “very common,” Dr. Pierre Kory says.


The following information is based on a report originally published by A Midwestern Doctor. Key details have been streamlined and editorialized for clarity and impact. Read the original report here.
They mocked this as a “conspiracy theory.”
Now the evidence shows that shedding from the COVID jab isn’t just real.
It’s “VERY COMMON,” Dr. Pierre Kory says.
“Everybody thinks it’s only the unvaccinated who are screaming [about shedding]... That’s not true.”
“I have vaccine-injured patients who are sensitive to being exposed to other vaccinated [people].”
“I think shedding is very common.”
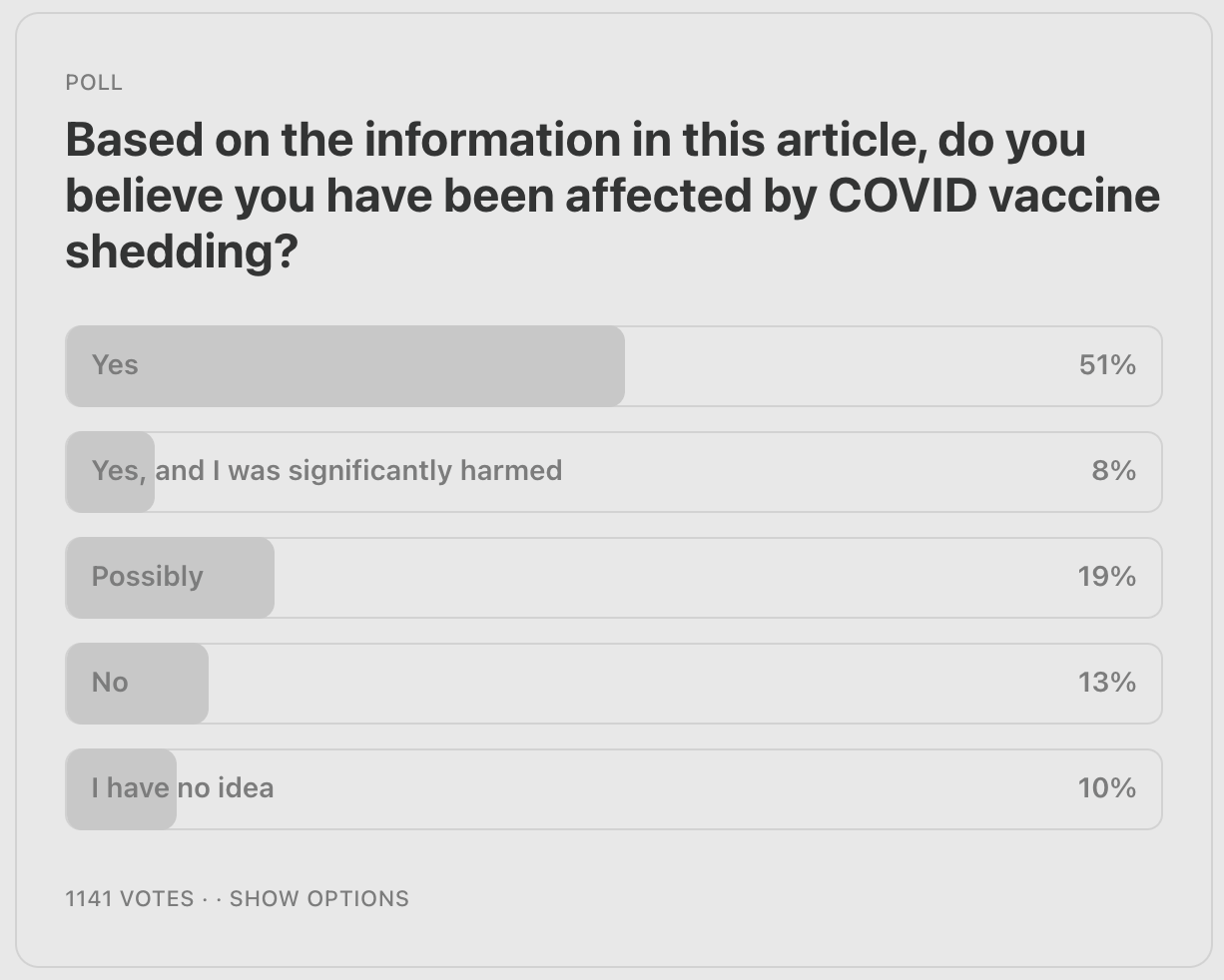
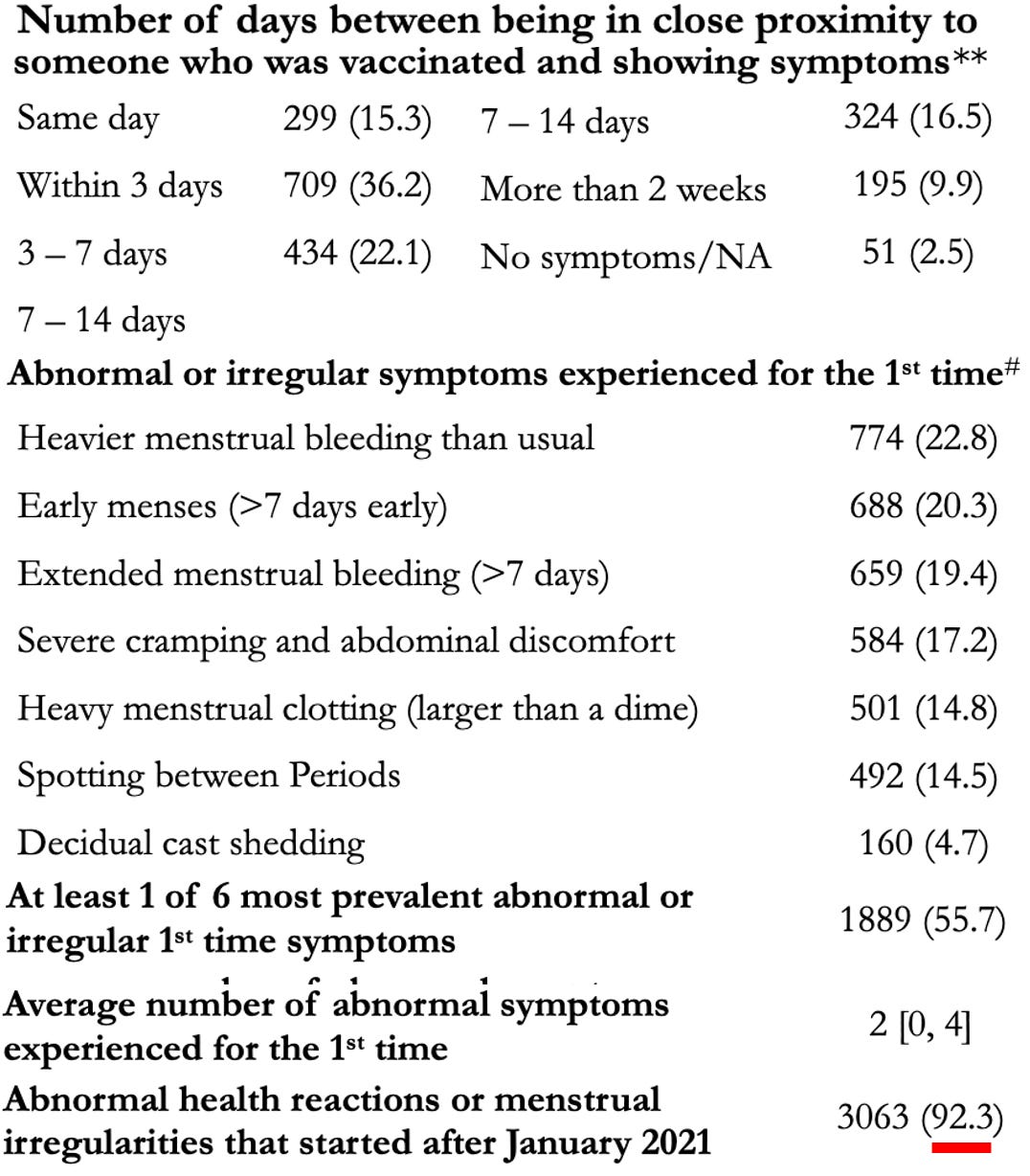
A survey of 6,049 women found that 92.3% reported unusual reactions or changes to their menstrual cycle starting in early 2021.
That was right after the jab rollout.
Many said the symptoms began within three days of being around someone who had recently been vaccinated.
Another disturbing pattern emerged among unvaccinated children living with vaccinated parents.
Shedding is “conspiracy theory” no more. Here’s the evidence they don’t want you to see.
For years, anyone who even questioned whether COVID vaccine shedding was possible or not was treated like a crazy conspiracy theorist.
“Impossible,” we were told. “It doesn’t contain live virus. mRNA can’t replicate.”
But that elephant in the room has refused to go away.
But thousands of reports and a clear patter continue to tell us that COVID vaccine shedding is very, very real.

After the vaccine rollout, unvaccinated people began reporting something strange and deeply unsettling.
They weren’t just getting sick. They were getting sick after close contact with recently vaccinated people.
Not randomly. Not vaguely.
Repeatedly.
That’s when this stopped being noise and started being a pattern.

This information comes from the work of medical researcher A Midwestern Doctor. For all the sources and details, read the full report below.
What We Now Know About COVID Vaccine Shedding

What makes this different isn’t one dramatic story.
It’s the volume of reports.
Roughly 1,500 case reports were compiled.
Different states. Different professions. Different political views.
But the symptom clusters kept repeating. It was consistent.
At what point does a repeated pattern deserve examination?
The symptoms aren’t vague.
Menstrual disruption.
Headaches.
Nosebleeds.
Flu-like illness.
Tinnitus.
Rashes.
Palpitations.
And in many cases—the onset followed proximity within hours or days.

The most commonly reported effect wasn’t mild fatigue or a headache. It was menstrual disruption. Not mild irregularity.
Heavier bleeding.
Early cycles.
Extended cycles.
Large clots.
Postmenopausal bleeding in women who hadn’t menstruated for decades.
The pattern became difficult to ignore. But women were repeatedly ignored or called crazy if they dare bring it up. As if they were unfamiliar with their own bodies and own cycles.

An IRB-approved MyCycleStory survey of 6,049 women found that 92.3% reported abnormal health reactions or menstrual irregularities that began after January 2021.
Ninety-two percent.
Many reported onset within three days of exposure to vaccinated people.
Three days.
And proximity appeared to matter.
Something was clearly happening and it didn’t have anything to do with confused or paranoid women. It was real.
The data showed something else. Relative risk increased in women who:
Lived with vaccinated partners
Were within six feet of vaccinated people daily
Or had frequent close contact with vaccinated people
The closer and more sustained the exposure—the higher the reported abnormality rate.
But why would distance matter if nothing biological is transferring?
They tried to keep us six feet apart to stop the spread of COVID. But maybe the unvaccinated should have stayed six feet away from the vaccinated.

Most shockingly, postmenopausal bleeding was repeatedly reported.
Women who had not menstruated for decades suddenly experienced cramping and hemorrhage after close exposure.
Women who had undergone hysterectomy reported severe cramping.
Girls as young as 8–9 reportedly experienced abnormal bleeding.
In some cases, bleeding was severe enough to require emergency care.
Imagine walking into a clinic and being told it’s just stress.
Would you accept that?

The full report goes much deeper into the most disturbing menstrual cases—including decidual cast shedding, hemorrhage events, and the biological mechanisms proposed to explain them.
Subscribe to A Midwestern Doctor to access the full breakdown.
What We Now Know About COVID Vaccine Shedding
Beyond menstruation, other bleeding patterns appeared.
Unexplained bruising.
Frequent nosebleeds.
Gums bleeding.
Even conjunctival hemorrhages.
And platelet crashes in individuals with previously stable counts.
Is psychosomatic stress known to cause platelet levels to plummet below 2,000? Or are we ignoring that elephant in the room?

Then came the inflammatory cascade.
Severe pressure headaches described as “nail-through-the-temple” pain.
Neck stiffness.
Swollen lymph nodes.
Fatigue lasting days or weeks.
Often beginning within 6–24 hours of exposure.
If this is anxiety, why is the onset so physiologically consistent?

Neurological symptoms followed similar patterns:
Tinnitus.
Dizziness.
Brain fog.
Internal vibrations.
Peripheral neuropathy.
Many mirrored known post-vaccine injury profiles.
The overlap is uncomfortable, but ignoring it doesn’t make it go away.

Cardiac symptoms were also reported.
Chest tightness.
Arrhythmias.
Tachycardia.
PVCs.
A smaller number described myocarditis-like symptoms and clotting events.
Are we willing to even ask whether proximity could trigger inflammatory cardiac stress in susceptible individuals?
Can you imagine avoiding the injections because you knew these symptoms were possible… only to experience them anyway?

Immune suppression patterns appeared as well.
Things like:
Shingles reactivation.
Herpes flares.
Epstein–Barr reactivation.
Chronic susceptibility to illness.
The symptom cluster looked less like coincidence—and more like biological stress.
And if it is biological stress, what is driving it?

Now here’s the mechanistic wall everyone hides behind: “mRNA doesn’t replicate.”
True. But shedding doesn’t require viral replication in the classic sense.
So… what could be transferring?
Let’s look at three possible mechanisms.

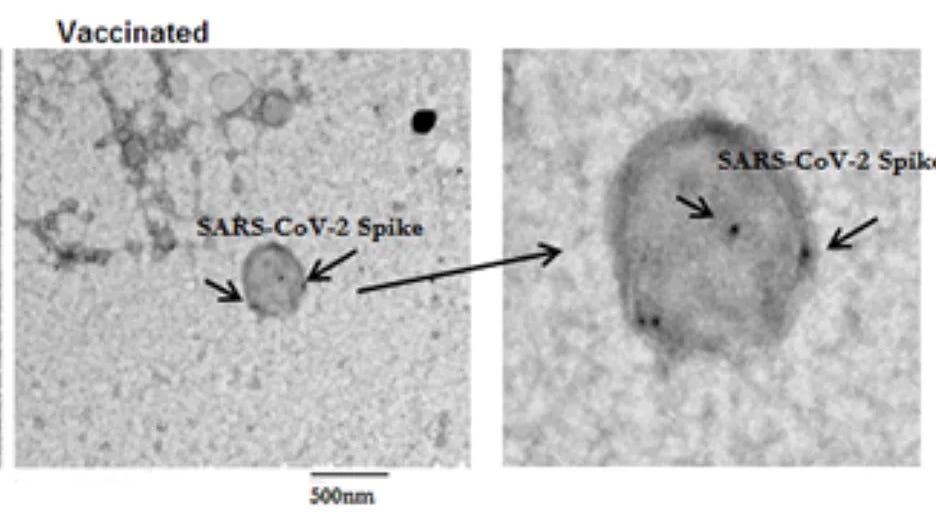
Mechanism #1: Exosomes
Cells release microscopic vesicles that can carry proteins and RNA.
Studies show spike-protein-containing exosomes increase after vaccination and circulate in the blood.
Exosomes are also present in breath.
They can be inhaled. They can interact with lung tissue.
If spike-bearing exosomes are exhaled, is inhalation really biologically implausible?
A 2023 peer-reviewed study found unvaccinated children living with vaccinated parents developed antibodies to spike protein—despite not being vaccinated.
Spike-related immune activity was detected in masks worn by physicians.
It sure seems like something was being transferred.

Mechanism #2: Increased SARS-CoV-2 transmission
Vaccinated individuals do not develop strong mucosal IgA immunity in the respiratory tract.
That means respiratory colonization remains possible—even if symptoms aren’t present.
Reduced symptoms does not equal reduced spread.
Sounds a bit like asymptomatic spread, doesn’t it? Except it’s not the unvaccinated people doing the spreading.

Mechanism #3: Plasmid contamination
Manufacturing processes introduced synthetic bacterial DNA fragments into some vaccine lots.
If those fragments integrate into microbiome bacteria, in theory they could replicate and spread.
This remains speculative—but biologically plausible.
Speculative is not the same as impossible.

One of the most concerning and controversial claims involves sexual exposure.
Reports describe severe menstrual disruption, bleeding, gastrointestinal distress, and cardiac symptoms following intimate contact with a vaccinated partner.
The closer the contact—the stronger the reported reaction.
Why would intimacy amplify effects? Because dose matters.

Some people have reported ending relationships over it. And some reported becoming severely ill after unprotected intercourse.
Others described months of cycle disruption following repeated intimate contact.
How many of these stories remain private?
How many never get reported?

The full report from A Midwestern Doctor includes detailed case reports on sexual shedding—including severe menstrual disruption, cardiac events, and intimate exposure patterns that are far more detailed and explicit than what’s covered here.
What We Now Know About COVID Vaccine Shedding
There are also accounts of aggressive cancers appearing shortly after repeated close exposure.
The sample size is small. But the timing patterns are troubling enough to raise the question.
Cancer rates have spiked since 2021.
Is shedding part of that equation?
We don’t know. But refusing to study it or even ask the question ensures we never will.

Blood transfusions are another concern.
Theoretically, red blood cells cannot produce spike protein. And white blood cells are typically removed before transfusion.
That suggests transfusion-related injury risk—if present—would likely be rare and temporary.
But if circulating spike protein exists in donor blood — even temporarily — what happens in highly sensitive recipients?
Rare does not mean zero.
The full article also examines aggressive cancer cases, blood transfusion risks, and specific mitigation protocols.
If you want the complete analysis and protocols, subscribe to A Midwestern Doctor.
What We Now Know About COVID Vaccine Shedding
Some mitigation strategies have been reported. They include:
Proteolytic enzymes
Nattokinase
Bromelain
Quercetin
Disinfection protocols
Some report improvement and relief while others report none.
Sensitivity appears highly individualized. Why are some individuals highly reactive while others feel nothing?
Genetics? Immune priming? Microbiome differences?
That variability itself suggests biology—not something we should dismiss as mass hysteria.

This isn’t about division. It’s about regulatory consistency.
Every other gene therapy must undergo formal shedding evaluation.
If mRNA technology behaves similarly, that standard should apply here too.
Why was it mass-deployed without comparable shedding analysis?
That question isn’t fringe. It isn’t extreme.
It’s procedural, and it’s fair.

Here’s the bottom line:
When 1,500 case reports cluster, when structured surveys show temporal spikes, and when peer-reviewed studies detect antibody formation in unvaccinated household contacts.
You don’t dismiss it. You investigate it.
Because if shedding is real—even in a subset of people—it changes everything.

Thanks for reading! This information was based on a report originally published by A Midwestern Doctor. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
What We Now Know About COVID Vaccine Shedding
For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by A Midwestern Doctor:
Statins, Cholesterol, and The Real Cause of Heart Disease
What’s The Healthiest Water To Drink?
The Unsettling Brain Impact of Screen Time in Kids
While you’re at it, give A Midwestern Doctor a follow. No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed. This is easily one of the most valuable accounts you’ll ever follow.

If you haven’t subscribed to this Substack yet, take a moment to read what some of the most powerful voices in the medical freedom/truth movement have to say:
“The Vigilant Fox has been putting in a lot of work to create a news platform that shares the stories we want to hear about and brings attention to the most important things to know about.”
– A Midwestern Doctor, The Forgotten Side of Medicine
“The Vigilant Fox absolutely is on top of things. We must support our fighters, and the Fox is fighting with truth.”
– Tom Renz, Tom Renz’s Newsletter
“Excellent capture of key video presentations on evolving pandemic science.”
– Peter A. McCullough, MD, MPH, FOCAL POINTS (Courageous Discourse)

I have a question. Was any of this cross referenced with the roll out of 5G & Cell towers because these symptoms also can be caused by EMF radiation. Cell towers have nothing to do with increased cellular phone coverage & everything to do with killing you and activating the nanobots inside you from the said mRNA vxeens & from the toxic cloud seeding/geoengineering that is taking place above our heads on a daily basis.
My husband got vaccinated and I did not. The two years following his vaccinations I developed trigeminal neuralgia, fluid on my heart and I was hospitalized for a blood clot. I put it all together about a year ago. I’m still fighting some of the symptoms.