
Carpal Tunnel May Not Be Caused by Overuse After All
Millions are treating the symptoms. Few are asking why the pressure builds in the first place.


The following information is based on a report originally published by A Midwestern Doctor. Key details have been streamlined and editorialized for clarity and impact. Read the original report here.
A registered nurse with 30 years of experience treating chronic pain says she saw “TEN TIMES” the positive effects after combining DMSO with castor oil for her peripheral neuropathy.
Castor oil already has anti-inflammatory properties.
But adding DMSO is where she says it “got interesting.”
That’s because DMSO “isn’t just a treatment, it’s a carrier,” Danielle Minetti explained.
“It can pull medications and nutrients right through the skin barrier deep into the body.”
When Danielle combined it with castor oil, she says the results increased “ten times.”
DMSO acted as the delivery system, carrying the castor oil deeper into the areas where she needed relief most.
But DMSO’s potential extends far beyond peripheral neuropathy.
And if you’re one of the 5 million Americans living with carpal tunnel syndrome, this is where the DMSO story gets really interesting.
Because it turns out carpal tunnel may not be caused by overuse after all.
Somewhere between the wrist pain that shows up after years of typing and the keyboard sitting under your fingers right now, there’s a design decision nobody remembers making.
It wasn’t an accident. It was a deliberate engineering choice made to solve a mechanical problem.
But that problem that stopped mattering almost a century ago. And the fix that’s still shaping our hands today has far outlived it.
Early typewriters had a real problem: type two adjacent keys too quickly and the mechanism would jam.
The fix was mechanical, not electronic. Spread the commonly paired letters as far apart as possible so fingers physically couldn’t hit them fast enough to jam the machine.
That layout is the same one you’re using right now.
That was over a century ago.
Mechanical jamming stopped being a problem once electric typewriters showed up. Computers can’t jam at all.
But the keyboard never changed.

In the 1930s, an educational psychologist named August Dvorak advised a master’s thesis on typing errors. What he found convinced him the standard layout wasn’t just outdated, it was actively working against speed, accuracy, and hand fatigue.
So he decided to build something better.
Dvorak and his brother-in-law spent years designing an alternative.
Common letters sit on the home row, so fingers barely have to travel. Frequently paired keys sit close together instead of far apart. The two hands trade off letter by letter instead of one hand doing most of the work.
Laid side by side with the old layout, the difference in finger travel is obvious.
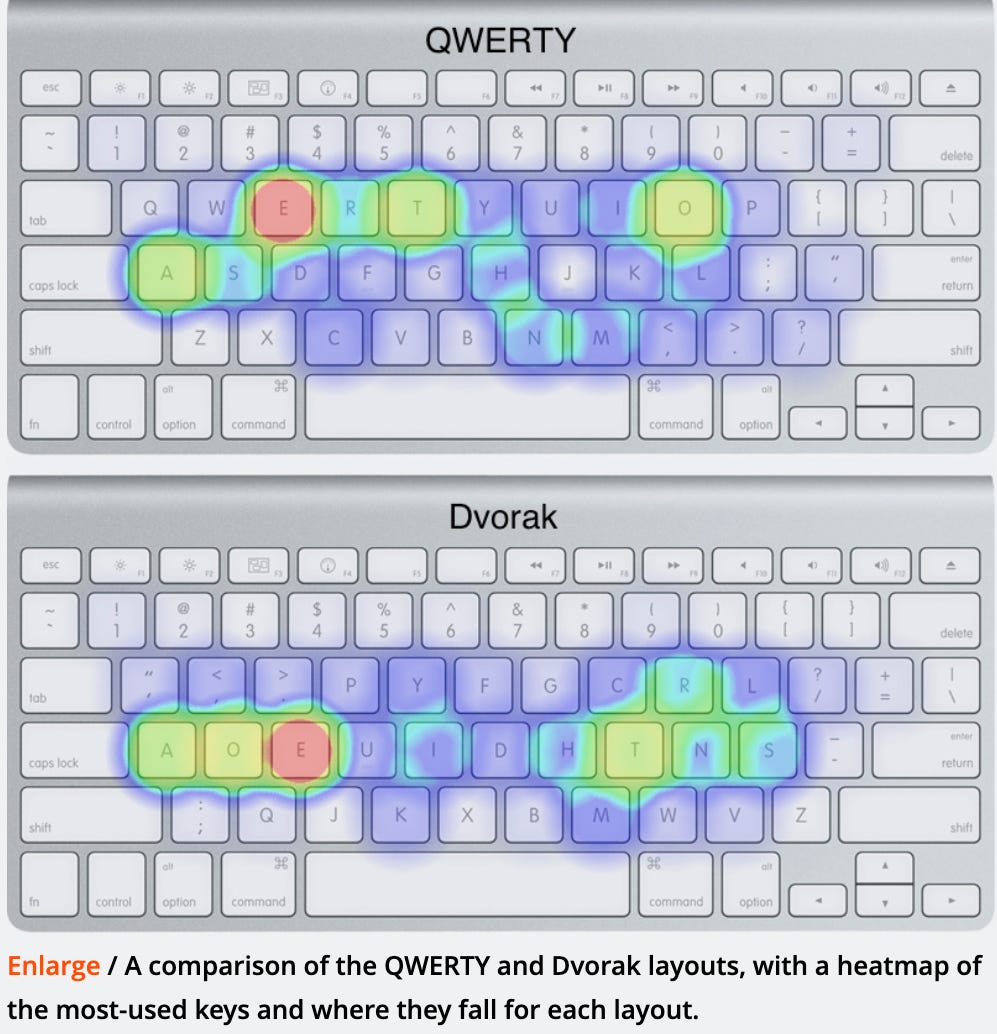
The two keyboards went head to head.
One had already won the market by accident, built decades earlier to slow typists down so fragile machines wouldn’t jam. The other was engineered from the ground up to be faster, more accurate, less punishing on the hands.
The better one lost.

From the fight between these two keyboards, to a wrist injury nobody expected, A Midwestern Doctor’s full piece connects the two in a way that’s easy to miss once you’re not looking for it.
The Forgotten History of Carpal Tunnel Syndrome

Stories like this rarely stay contained to keyboards.
A market settles on a standard, the standard gets defended by habit instead of performance, and the accumulated cost gets paid quietly, one body at a time.

Nowhere absorbs that kind of quiet cost more than the wrist.
Carpal tunnel syndrome is one of the most common reasons people end up in a doctor’s office with wrist pain and numbness in the fingers.
The typical progression looks like this: nighttime wrist splinting to reduce nerve pressure, ergonomic adjustments to cut repetitive strain, short courses of anti-inflammatories, corticosteroid injections directly into the tunnel for swelling, physical therapy, and if none of that works, surgery to cut open the ligament that forms the roof of the tunnel.
Six steps. All of them mechanical.
Every single one of those steps manages pressure or masks pain.
Not one of them asks why the pressure built up inside the tunnel in the first place.
And a striking number of patients who go all the way to surgery come out the other side no better than before.

Curiously, pregnant women develop carpal tunnel for the first time at a strikingly high rate, and it lines up almost exactly with a body-wide increase in fluid retention during pregnancy.
That’s not a coincidence. It suggests the real driver of carpal tunnel probably isn’t tissue damage from overuse. It’s fluid that has nowhere to drain, trapped inside a narrow anatomical tunnel.

If fluid pressure really is the root cause, then the fix isn’t cutting the ligament open. It’s restoring the fluid movement that broke down in the first place.
That’s the exact reason some are trying a decades-old topical compound called DMSO. It’s known for an unusual ability to move through tissue and influence fluid exchange at the cellular level, which is precisely the mechanism in question here.
None of this is a fringe idea being floated for the first time. Topical DMSO carries decades of published research on tunnel neuropathies, formal clinical guidelines for carpal tunnel already exist in Russia, and reader accounts, including cases where surgery had already failed, have been remarkably consistent.

The full physiological explanation for why fluid circulation breaks down in the first place, and what’s been shown to restore it, is laid out in a companion piece on DMSO from A Midwestern Doctor that reads like the missing chapter to this one.
How DMSO Heals The Nerves & Eliminates Pain

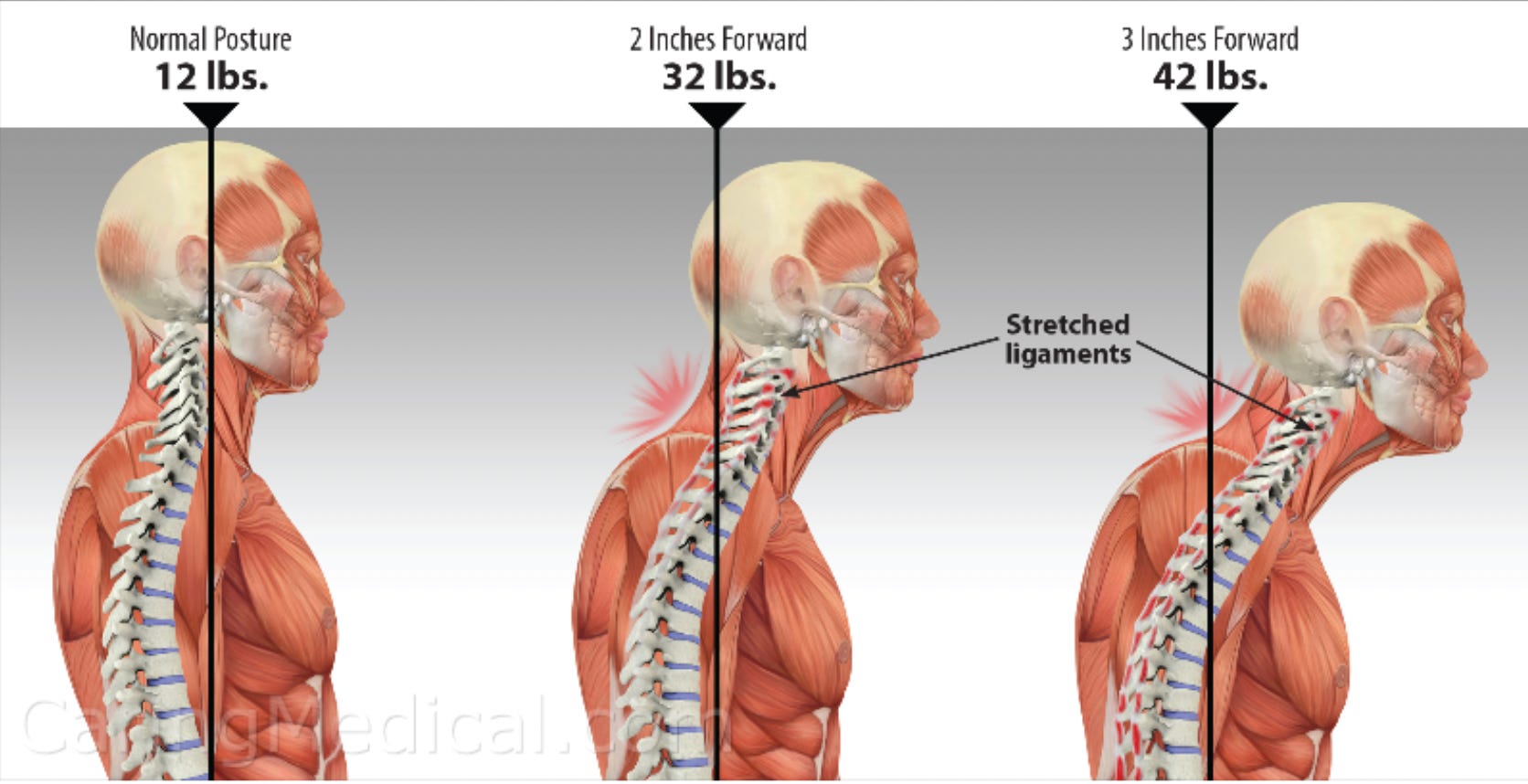
Let’s consider posture. At a neutral, upright position, the average human head puts about 12 pounds of load on the neck.
Lean the head forward two inches, the load roughly triples. Lean it three inches, and it’s closer to four times the starting load.
That’s not a subtle shift. That’s the physics behind every hour spent hunched toward a laptop.
The fixes people land on tend to fall into a handful of categories: raising a monitor to eye level, a slow-speed treadmill desk, a standing desk, or a supported squatting position instead of sitting.
None of them is universally “the” answer. That’s exactly why so many competing camps each insist their fix is the only real one.

The body has a threshold for how much strain it can absorb before damage starts accumulating instead of resolving on its own. Most people don’t notice they’ve crossed it until they’re already in pain.
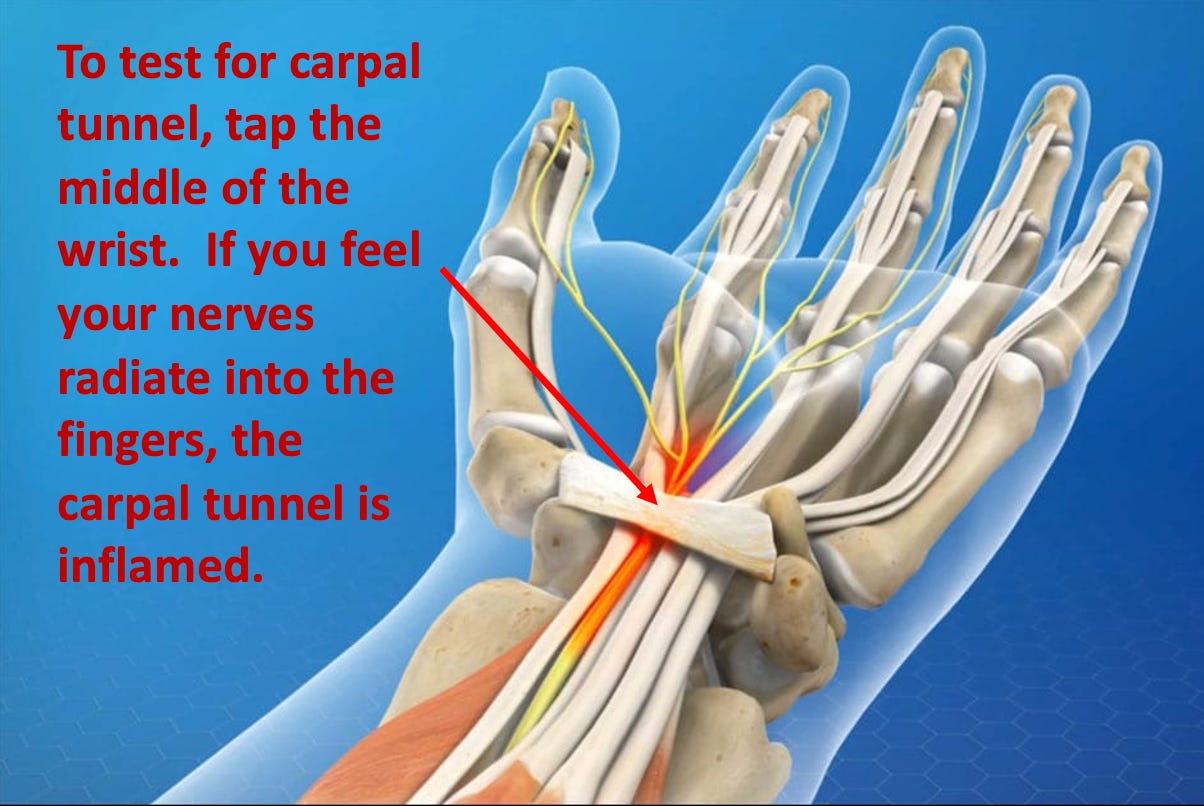
There’s a simple early warning test: tap the middle of the wrist, over the carpal tunnel itself. If the nerves fire and you feel it radiate into your fingers, that tunnel is already inflamed, often well before any overt pain or numbness shows up.
Catching it at that stage is dramatically easier to reverse than waiting until typing itself becomes impossible.

The free version of this article stops right at the edge of the actual fix. What’s behind it: the specific at-home protocol for reversing carpal tunnel at its root, plus the exact way DMSO gets applied for it. It is worth subscribing for.
The Forgotten History of Carpal Tunnel Syndrome
Widen the lens and a pattern shows up everywhere.
Keyboards, chairs, desks, and even treatment algorithms are often just inherited defaults, built for constraints that stopped existing decades ago, and rarely questioned because “that’s just how it’s done.”
Carpal tunnel syndrome turns out to be a small example of a much bigger habit.

The same quiet inertia that kept an inferior keyboard in place for a hundred years is still running in the background of how pain gets treated.
Nobody designed it maliciously. Nobody voted for it. It will keep costing people comfort, money, and function until someone asks the one question none of the standard steps ever get around to asking.
Why was the pressure there in the first place.

Thanks for reading! This information was based on a report originally published by A Midwestern Doctor. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
The Forgotten History of Carpal Tunnel Syndrome
For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by A Midwestern Doctor:
We Now Know How The Government Lied About the COVID Vaccines
The Hidden Dangers of Hospital Births & How to Protect Your Family
What’s The Healthiest Water To Drink?

While you’re at it, give A Midwestern Doctor a follow. No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed. This is easily one of the most valuable accounts you’ll ever follow.
If you haven’t subscribed to this Substack yet, take a moment to read what some of the most powerful voices in the medical freedom/truth movement have to say:
“The Vigilant Fox has been putting in a lot of work to create a news platform that shares the stories we want to hear about and brings attention to the most important things to know about. If you want a daily newsfeed in alignment with our ...”
– A Midwestern Doctor, The Forgotten Side of Medicine
“The Vigilant Fox absolutely is on top of things. We must support our fighters, and the Fox is fighting with truth.”
– Tom Renz, Tom Renz’s Newsletter
“Excellent capture of key video presentations on evolving pandemic science.”
– Peter A. McCullough, MD, MPH, FOCAL POINTS (Courageous Discourse)

I read if you use Botox the DMSO will take it away from where it was injected, is this true?
Is the castor oil/DMSO applied topically or taken internally?